

Review
doi: 10.1172/JCI29024.
Insulin resistance and atherosclerosis
Affiliations
- PMID: 16823479
- PMCID: PMC1483180
- DOI: 10.1172/JCI29024
Item in Clipboard
Review
Insulin resistance and atherosclerosis
J Clin Invest.
2006 Jul.
Abstract
Considerable evidence supports the association between insulin resistance and vascular disease, and this has led to wide acceptance of the clustering of hyperlipidemia, glucose intolerance, hypertension, and obesity as a clinical entity, the metabolic syndrome. While insulin resistance, by promoting dyslipidemia and other metabolic abnormalities, is part of the proatherogenic milieu, it is possible that insulin resistance itself in the vascular wall does not promote atherosclerosis. Recent findings suggest that insulin resistance and atherosclerosis could represent independent and ultimately maladaptive responses to the disruption of cellular homeostasis caused by the excess delivery of fuel.
Figures
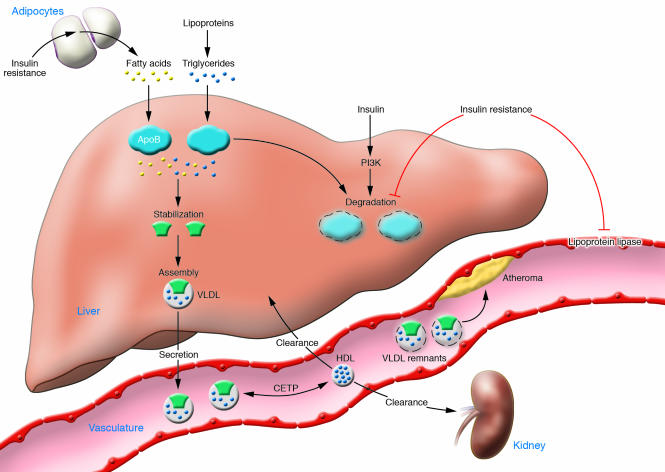
Early in the course of systemic insulin resistance, FFAs increase because of loss of the suppressive effects of insulin on lipolysis in adipocytes. Fatty acids are transported to the liver, where the availability of lipid stabilizes the production of apoB, the major apolipoprotein of VLDL particles. Decreased insulin signaling dampens degradative pathways for apoB, which also contributes to increased VLDL production. Lipoprotein lipase, found in the endothelium of peripheral capillaries and rate-limiting for the clearance of triglyceride-rich lipoproteins, is decreased in insulin resistance. Hence, hypertriglyceridemia in insulin resistance (reflecting elevated VLDL particles) occurs because of a combination of increased VLDL production and decreased VLDL clearance. VLDLs are metabolized to remnant lipoproteins, which can promote atheroma formation. The presence of increased VLDL particles also affects HDL metabolism. Triglycerides in VLDL are transferred to HDL through the action of cholesteryl ester transfer protein (CETP). This process results in a triglyceride-enriched HDL particle that is more rapidly cleared from the circulation, leaving fewer HDL particles to accept cholesterol from the vasculature.
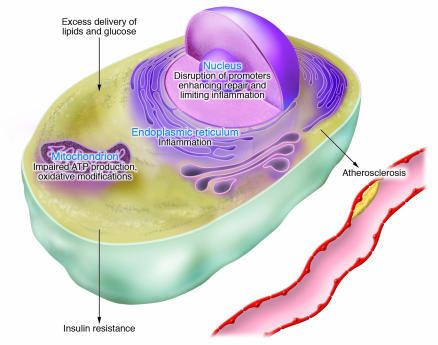
The excess delivery of glucose, lipids, and other nutrients disrupts homeostasis at key organelles, leading to genomic and ER stress. Increased fuel flow is associated with increased mitochondrial metabolism with the potential for excessive generation of reactive oxygen species, leading to mitochondrial dysfunction. The nuclear genome may be affected by oxidative modifications and by structural alterations due to the accumulation of intracellular lipids, both of which may disrupt repair mechanisms as well as transcriptional responses that minimize inflammatory damage. Excessive demand on the ER induces stress responses that lead to inflammation. Genomic and ER stress could be adaptive in the short term, since decreased insulin signaling would limit additional uptake of nutrients and increased macrophage activation would clear toxic lipids. However, these independent processes stimulated by organelle stress ultimately become maladaptive in the setting of continued nutrient excess.
References
-
- Enzi G., Busetto L., Inelmen E.M., Coin A., Sergi G. Historical perspective: visceral obesity and related comorbidity in Joannes Baptista Morgagni’s ‘De sedibus et causis morborum per anatomen indagata.’. Int. J. Obes. Relat. Metab. Disord. 2003;27:534–535. - PubMed
-
- Himsworth H. The mechanism of diabetes mellitus. III. Human diabetes mellitus. Lancet. 1939;2:171–175.
-
- Albrink M.J., Mann E.B. Serum triglycerides in coronary artery disease. Trans. Assoc. Am. Physicians. 1958;71:162–173. - PubMed
-
- Reaven G., Calciano A., Cody R., Lucas C., Miller R. Carbohydrate intolerance and hyperlipemia in patients with myocardial infarction without known diabetes mellitus. J. Clin. Endocrinol. Metab. 1963;23:1013–1023. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
