

Randomised controlled trial of near-patient testing for glycated haemoglobin in people with type 2 diabetes mellitus
- PMID: 16834877
- PMCID: PMC1872061
Randomised controlled trial of near-patient testing for glycated haemoglobin in people with type 2 diabetes mellitus
Abstract
Background: Tight glycaemic control in people with type 2 diabetes can lead to a reduction in microvascular and possibly macrovascular complications. The use of near-patient (rapid) testing offers a potential method to improve glycaemic control.
Aim: To assess the effect and costs of rapid testing for glycated haemoglobin (HbA1c) in people with type 2 diabetes.
Design of study: Pragmatic open randomised controlled trial.
Setting: Eight practices in Leicestershire, UK.
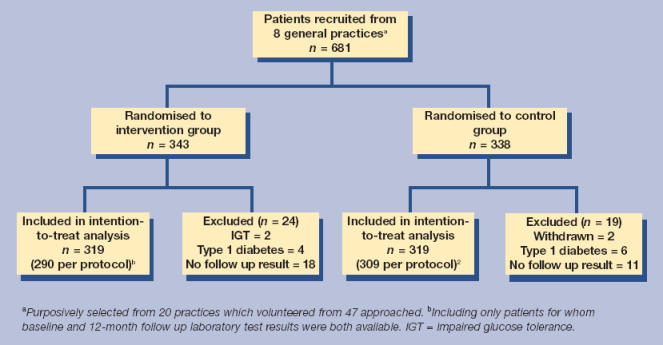
Method: Patients were randomised to receive instant results for HbA1c or to routine care. The principal outcome measure was the proportion of patients with an HbA1c <7% at 12 months. We also assessed costs for the two groups.
Results: Of the 681 patients recruited to the study 638 (94%) were included in the analysis. The mean age at baseline was 65.7 years (SD = 10.8 years) with a median (interquartile range) duration of diabetes of 4(1-8) years. The proportion of patients with HbA1c < 7% did not differ significantly between the intervention and control groups (37 versus 38%, odds ratio 0.95 [95% confidence interval = 0.69 to 1.31]) at 12 months follow up. The total cost for diabetes-related care was 390 UK pounds per patient for the control group and 370 UK pounds for the intervention group. This difference was not statistically significant.
Conclusion: Near-patient testing for HbA1c alone does not lead to outcome or cost benefits in managing people with type 2 diabetes in primary care. Further research is required into the use of rapid testing as part of an optimised patient management model including arrangements for patient review and testing.
Figures
Similar articles
-
Near patient testing for glycated haemoglobin in people with Type 2 diabetes mellitus managed in primary care: acceptability and satisfaction.Diabet Med. 2007 Jul;24(7):792-5. doi: 10.1111/j.1464-5491.2007.02175.x. Epub 2007 Apr 19. Diabet Med. 2007. PMID: 17451419 Clinical Trial.
-
Structured, intensive education maximising engagement, motivation and long-term change for children and young people with diabetes: a cluster randomised controlled trial with integral process and economic evaluation - the CASCADE study.Health Technol Assess. 2014 Mar;18(20):1-202. doi: 10.3310/hta18200. Health Technol Assess. 2014. PMID: 24690402 Free PMC article. Clinical Trial.
-
Improving type 2 diabetes mellitus glycaemic outcomes is possible without spending more on medication: Lessons from the UK National Diabetes Audit.Diabetes Obes Metab. 2018 Jan;20(1):185-194. doi: 10.1111/dom.13067. Epub 2017 Sep 8. Diabetes Obes Metab. 2018. PMID: 28730750
-
Psychological interventions to improve self-management of type 1 and type 2 diabetes: a systematic review.Health Technol Assess. 2020 Jun;24(28):1-232. doi: 10.3310/hta24280. Health Technol Assess. 2020. PMID: 32568666 Free PMC article.
-
Repaglinide : a pharmacoeconomic review of its use in type 2 diabetes mellitus.Pharmacoeconomics. 2004;22(6):389-411. doi: 10.2165/00019053-200422060-00005. Pharmacoeconomics. 2004. PMID: 15099124 Review.
Cited by
-
Impact of HbA1c Testing at Point of Care on Diabetes Management.J Diabetes Sci Technol. 2017 May;11(3):611-617. doi: 10.1177/1932296816678263. Epub 2016 Nov 27. J Diabetes Sci Technol. 2017. PMID: 27898388 Free PMC article. Review.
-
How point-of-care HbA1c testing changes the behaviour of people with diabetes and clinicians - a qualitative study.Diabet Med. 2020 Jun;37(6):1008-1015. doi: 10.1111/dme.14219. Epub 2020 Jan 8. Diabet Med. 2020. PMID: 31876039 Free PMC article.
-
Economic Evidence and Point-of-Care Testing.Clin Biochem Rev. 2013 Aug;34(2):61-74. Clin Biochem Rev. 2013. PMID: 24151342 Free PMC article. Review.
-
Guidelines and Recommendations for Laboratory Analysis in the Diagnosis and Management of Diabetes Mellitus.Diabetes Care. 2023 Oct 1;46(10):e151-e199. doi: 10.2337/dci23-0036. Diabetes Care. 2023. PMID: 37471273 Free PMC article. Review.
-
Performance of Point-of-Care Testing Compared with the Standard Laboratory Diagnostic Test in the Measurement of HbA1c in Indonesian Diabetic and Nondiabetic Subjects.J Diabetes Res. 2020 Jul 9;2020:2037565. doi: 10.1155/2020/2037565. eCollection 2020. J Diabetes Res. 2020. PMID: 32733964 Free PMC article.
References
-
- Turner RC, Holman RR, Cull CA, et al. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352:837–853. - PubMed
-
- Shamoon H, Duffy H, Fleischer N, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–986. - PubMed
-
- Gilmer TP, O'Connor PJ, Manning WG, Rush WA. The cost to health plans of poor glycemic control. Diabetes Care. 1997;20:1847–1853. - PubMed
-
- Menzin JP, Langley-Hawthorne CML, Friedman MM, et al. Potential short-term economic benefits of improved glycemic control: a managed care perspective. Diabetes Care. 2001;24:51–55. - PubMed
-
- Wagner EH, Sandhu N, Newton KM, et al. Effect of improved glycemic control on health care costs and utilization. JAMA. 2001;285:182–189. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials