

Cardioprotective medication use in hemodialysis patients
- PMID: 16835669
- PMCID: PMC2560515
- DOI: 10.1016/s0828-282x(06)70291-4
Cardioprotective medication use in hemodialysis patients
Abstract
Background: Cardiovascular disease is the leading cause of mortality in patients with renal failure, accounting for more than 50% of deaths in end-stage renal disease. Risk factor modification with the use of cardioprotective medications such as angiotensin-converting enzyme inhibitors (ACEIs), beta-adrenergic antagonists (beta-blockers), acetylsalicylic acid (ASA) and 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors (statins) has been shown to reduce mortality in the general population.
Objective: To determine the extent of use of these medications in a hemodialysis population.
Methods: This was a cross-sectional study of a cohort of 185 prevalent hemodialysis patients. The inclusion criterion was dialysis dependence and there were no exclusion criteria. Data collection was by chart review. Contraindications to individual medication classes were not obtained.
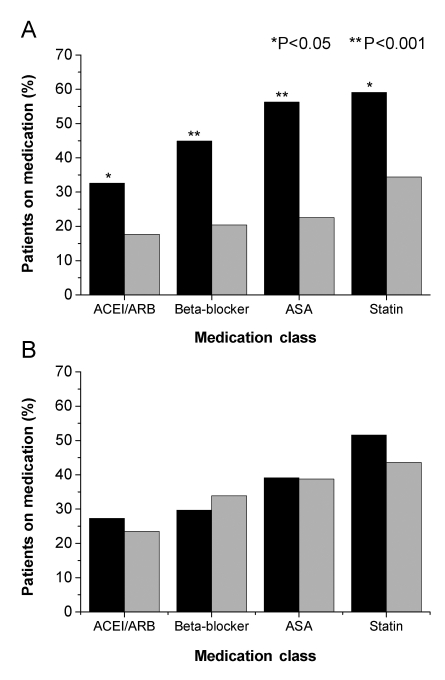
Results: There were 185 patients enrolled, the mean age was 63.42+/-15.1 years and 126 (68.1%) were male. Sixty-six (35.7%) patients had diabetes and 89 (48.1%) patients had established coronary artery disease (CAD). Forty-six (24.9%) patients were on ACEIs or angiotensin II receptor blockers, 59 (31.9%) were on beta-blockers, 70 (37.8%) were on ASA and 84 (45.4%) were on statins. Although these medications were used in fewer than 60% of patients, those with CAD were more likely to be prescribed an ACEI or an angiotensin II receptor blocker (P=0.026), a beta-blocker (P<0.001), ASA (P<0.001) or a statin (P=0.001) than those without CAD. There were no differences in the use of these medications between diabetic and nondiabetic patients.
Conclusions: Many hemodialysis patients are not prescribed cardioprotective medications. Given the high cardiovascular mortality in this high-risk population, more attention to reducing cardiovascular risk is warranted.
HISTORIQUE: Les maladies cardiovasculaires sont la principale cause de mortalité chez les patients atteints d’insuffisance rénale, représentant plus de 50 % des décès en cas d’insuffisance rénale terminale. Il est démontré que la modification des facteurs de risque grâce à des médicaments cardioprotecteurs comme des inhibiteurs de l’enzyme de conversion de l’angiotensine (IECA) des antagonistes béta-adrénergiques (béta-bloquants), de l’acide acétylsalicylique (ASA) et des inhibiteurs de la 3-hydroxy-3-méthylglutaryl coenzyme A réductase (statines) réduit le taux de mortalité dans la population générale.
OBJECTIF: Déterminer la portée de l’utilisation de ces médicaments au sein de la population des hémodialysés.
MÉTHODOLOGIE: Il s’agissait de l’étude transversale d’une cohorte de 185 hémodialysés prévalents. Les critères d’inclusion étaient la dépendance à la dialyse. Il n’y avait pas de critères d’exclusion. La collecte de données s’est effectuée par analyse des dossiers. On n’a pas obtenu les contre-indications aux classes de médicaments.
RÉSULTATS: Cent quatre-vingt-cinq patients ont participé, d’un âge moyen de 63,42±15,1 ans, dont 126 (68,1 %) étaient de sexe masculin. Soixante-six (35,7 %) étaient diabétiques et 89 (48,1 %) souffraient d’une coronaropathie établie. Quarante-six patients (24,9 %) prenaient des IECA ou des antagonistes de l’angiotensine II, 59 (31,9 %), des béta-bloquants, 70 (37,8 %), de l’ASA et 84 (45,4 %), des statines. Même si moins de 60 % des patients prenaient ces médicaments, ceux atteints d’une coronaropathie étaient plus susceptibles d’avoir une prescription d’IECA ou d’antagonistes de l’angiotensine II (P=0,026), de béta-bloquants (P<0,001), d’ASA (P<0,001) ou de statines (P=0,001) que ceux qui n’avaient pas de coronaropathie. Il n’y avait pas de différence d’usage de ces médicaments chez les diabétiques et les non-diabétiques.
CONCLUSIONS: De nombreux hémodialysés n’ont pas de prescription de médicaments cardioprotecteurs. Étant donné le taux élevé de mortalité cardiovasculaire au sein de cette population très vulnérable, il faut accorder plus d’attention à la réduction du risque cardiovasculaire.
Figures
References
-
- Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32(5 Suppl 3):S112–9. - PubMed
-
- Longenecker JC, Coresh J, Powe NR, et al. Traditional cardiovascular disease risk factors in dialysis patients compared with the general population: The CHOICE Study. J Am Soc Nephrol. 2002;13:1918–27. - PubMed
-
- Madore F. Uremia-related metabolic cardiac risk factors in chronic kidney disease. Semin Dial. 2003;16:148–56. - PubMed
-
- Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G Heart Outcomes Prevention Evaluation Study Investigators. Effects on angiotensin-converting enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 2000;342:145–53. - PubMed
-
- West of Scotland Coronary Prevention Study Group. Influence of pravastatin and plasma lipids on clinical events in the West of Scotland Coronary Prevention Study (WOSCOPS) Circulation. 1998;97:1440–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
