

Trends in market demand for internal medicine 1999 to 2004: an analysis of physician job advertisements
- PMID: 16836622
- PMCID: PMC1831623
- DOI: 10.1111/j.1525-1497.2006.00558.x
Trends in market demand for internal medicine 1999 to 2004: an analysis of physician job advertisements
Abstract
Background: The health care marketplace has changed substantially since the last assessment of demand for internal medicine physicians in 1996.
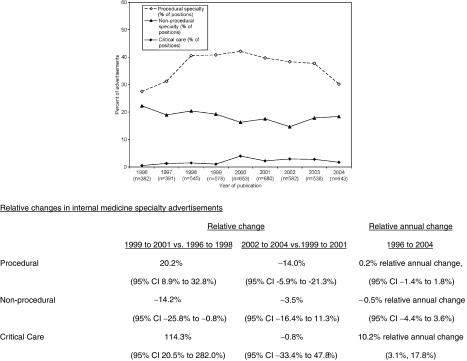
Methods: We reviewed internal medicine employment advertisements published in 4 major medical journals between 1996 and 2004. The number of positions, specialty, and other practice characteristics (e.g., location) were collected from each advertisement.
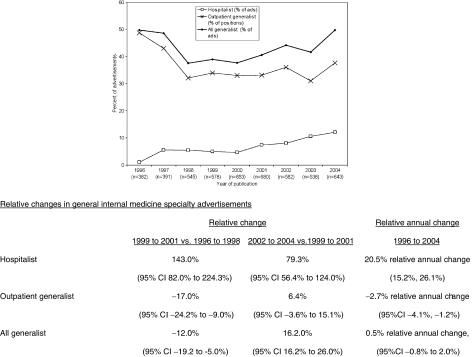
Results: Four thousand two hundred twenty-four advertisements posted 4,992 positions. Of these positions, jobs in the Northeast (31% of positions) or single specialty groups (36.8% of positions) were most common. The relative proportion of advertisements for nephrologists declined (P < .001), while the relative proportions of advertisements for critical care specialists (0.5% in 1996 to 1.7% in 2004, P = .004) and hospitalists (1.0% in 1996 to 12.1% in 2004, P < .001) increased. Advertisements for outpatient-based generalist positions (i.e., Primary Care and Internal Medicine) declined (-2.7% relative annual change, 95% confidence interval [95% CI] -4.1%, -1.2%) between 1996 and 2004, a decrease largely due to a substantial decline in advertisements noted between 1996 and 1998. However, over the entire time period, the combined proportion of advertisements for all generalists (hospitalists and outpatient-based generalists) did not change (0.5% relative annual change, 95% CI -0.8% to 2.0%).
Conclusions: Since 1996, demand for the majority of medical subspecialties has remained constant while relative demand has decreased for primary care and increased for hospitalists and critical care. Increase in demand for generalist-trained hospitalists appears to have offset falling demand for outpatient generalists.
Figures
References
-
- Greenfield S, Nelson EC, Zubkoff M, et al. Variations in resource utilization among medical specialties and systems of care. Results from the medical outcomes study. JAMA. 1992;267:1624–30. - PubMed
-
- Greenfield S, Rogers W, Mangotich M, Carney MF, Tarlov AR. Outcomes of patients with hypertension and non-insulin dependent diabetes mellitus treated by different systems and specialties. Results from the medical outcomes study. JAMA. 1995;274:1436–44. - PubMed
-
- Eisenberg JM. The internist as gatekeeper. Preparing the general internist for a new role. Ann Intern Med. 1985;102:537–43. - PubMed
-
- Auerbach AD, Hamel MB, Davis RB, et al. Resource use and survival of patients hospitalized with congestive heart failure: differences in care by specialty of the attending physician. SUPPORT investigators. Study to understand prognoses and preferences for outcomes and risks of treatments [see comments] Ann Intern Med. 2000;132:191–200. - PubMed
-
- Ayanian JZ, Guadagnoli E, McNeil BJ, Cleary PD. Treatment and outcomes of acute myocardial infarction among patients of cardiologists and generalist physicians. Arch Intern Med. 1997;157:2570–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources