

Prevalence and determinants of physician bedside rationing: data from Europe
- PMID: 16836629
- PMCID: PMC1831659
- DOI: 10.1111/j.1525-1497.2006.00551.x
Prevalence and determinants of physician bedside rationing: data from Europe
Abstract
Background: Bedside rationing by physicians is controversial. The debate, however, is clouded by lack of information regarding the extent and character of bedside rationing.
Design, setting, and participants: We developed a survey instrument to examine the frequency, criteria, and strategies used for bedside rationing. Content validity was assessed through expert assessment and scales were tested for internal consistency. The questionnaire was translated and administered to General Internists in Norway, Switzerland, Italy, and the United Kingdom. Logistic regression was used to identify the variables associated with reported rationing.
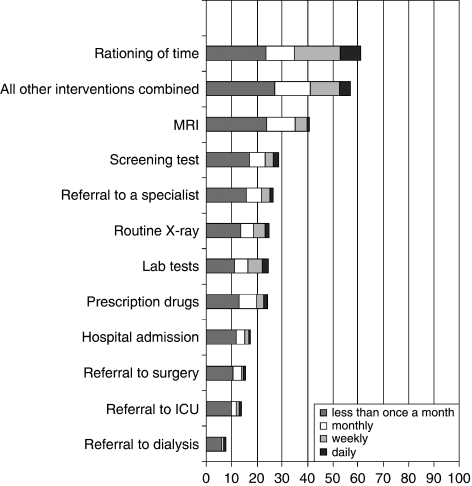
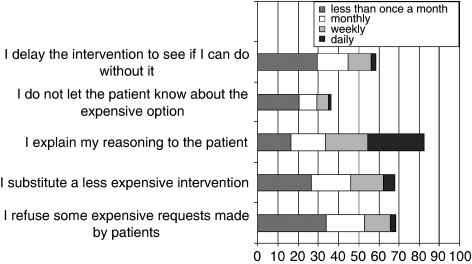
Results: Survey respondents (N=656, response rate 43%) ranged in age from 28 to 82, and averaged 25 years in practice. Most respondents (82.3%) showed some degree of agreement with rationing, and 56.3% reported that they did ration interventions. The most frequently mentioned criteria for rationing were a small expected benefit (82.3%), low chances of success (79.8%), an intervention intended to prolong life when quality of life is low (70.6%), and a patient over 85 years of age (70%). The frequency of rationing by clinicians was positively correlated with perceived scarcity of resources (odds ratio [OR]=1.11, 95% confidence interval [CI] 1.06 to 1.16), perceived pressure to ration (OR=2.14, 95% CI 1.52 to 3.01), and agreement with rationing (OR=1.13, 95% CI 1.05 to 1.23).
Conclusion: Bedside rationing is prevalent in all surveyed European countries and varies with physician attitudes and resource availability. The prevalence of physician bedside rationing, which presents physicians with difficult moral dilemmas, highlights the importance of discussions regarding how to ration care in the most ethically justifiable manner.
Figures
Comment in
-
Tough questions, even harder answers.J Gen Intern Med. 2006 Nov;21(11):1209-10. doi: 10.1111/j.1525-1497.2006.00617.x. J Gen Intern Med. 2006. PMID: 17026736 Free PMC article. No abstract available.
References
-
- Asch DA, Ubel PA. Rationing by any other name. N Engl J Med. 1997;336:1668–71. - PubMed
-
- Relman A. Use of medical resources—overview. Prev Med. 1990;19:688–92. - PubMed
-
- Bloche MG, Jungman ER. The “R” word. J Contemp Health Law Policy. 2002;18:633–9. - PubMed
-
- Coulter A, Ham C. The Global Challenge of Health Care Rationing. Buckingham: Open University Press; 2000.
-
- Sulmasy DP. Physicians, cost control, and ethics. Ann Intern Med. 1992;116:920–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources