

Impacts of evidence-based quality improvement on depression in primary care: a randomized experiment
- PMID: 16836631
- PMCID: PMC1831644
- DOI: 10.1111/j.1525-1497.2006.00549.x
Impacts of evidence-based quality improvement on depression in primary care: a randomized experiment
Abstract
Context: Previous studies testing continuous quality improvement (CQI) for depression showed no effects. Methods for practices to self-improve depression care performance are needed. We assessed the impacts of evidence-based quality improvement (EBQI), a modification of CQI, as carried out by 2 different health care systems, and collected qualitative data on the design and implementation process.
Objective: Evaluate impacts of EBQI on practice-wide depression care and outcomes.
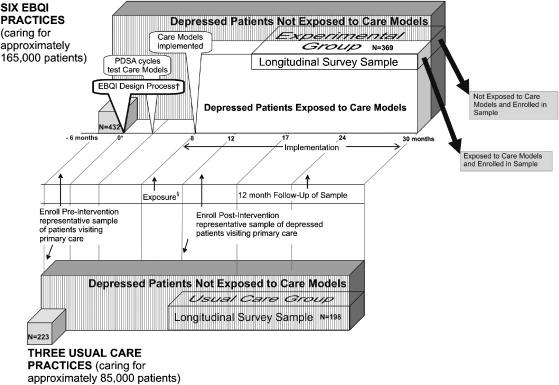
Design: Practice-level randomized experiment comparing EBQI with usual care.
Setting: Six Kaiser Permanente of Northern California and 3 Veterans Administration primary care practices randomly assigned to EBQI teams (6 practices) or usual care (3 practices). Practices included 245 primary care clinicians and 250,000 patients.
Intervention: Researchers assisted system senior leaders to identify priorities for EBQI teams; initiated the manual-based EBQI process; and provided references and tools. EVALUATION PARTICIPANTS: Five hundred and sixty-seven representative patients with major depression.
Main outcome measures: Appropriate treatment, depression, functional status, and satisfaction.
Results: Depressed patients in EBQI practices showed a trend toward more appropriate treatment compared with those in usual care (46.0% vs 39.9% at 6 months, P = .07), but no significant improvement in 12-month depression symptom outcomes (27.0% vs 36.1% poor depression outcome, P = .18). Social functioning improved significantly (mean score 65.0 vs 56.8 at 12 months, P = .02); physical functioning did not.
Conclusion: Evidence-based quality improvement had perceptible, but modest, effects on practice performance for patients with depression. The modest improvements, along with qualitative data, identify potential future directions for improving CQI research and practice.
Figures
Comment in
-
Depression in primary care: encouragement and caution for the business case.J Gen Intern Med. 2006 Oct;21(10):1125-7. doi: 10.1111/j.1525-1497.2006.00603.x. J Gen Intern Med. 2006. PMID: 16970563 Free PMC article. No abstract available.
References
-
- Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001. - PubMed
-
- Institute for the Future. Health and Health Care 2010: The Forecast, the Challenge. 2. New York: John Wiley & Sons; 2002.
-
- Schulberg HC, Katon W, Simon GE, Rush AJ. Treating major depression in primary care practice: an update of the agency for health care policy and research practice guidelines. Arch Gen Psychiatry. 1998;55:1121–7. - PubMed
-
- Depression Guideline Panel. Clinical Practice Guideline, Depression in Primary Care: Vol. 1. Detection and Diagnosis (AHCPR Publication No. 93-0550) Rockville, MD: U.S. Department of Health and Human Services, Public Health Service Agency for Health Care Policy and Research; 1993.
-
- Depression Guideline Panel. Clinical Practice Guideline, Depression in Primary Care: Vol. 2. Treatment of Major Depression (AHCPR Publication No. 93-0551) Rockville, MD: U.S. Department of Health and Human Services, Public Health Service Agency for Health Care Policy and Research; 1993.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical