

Effect of a lung recruitment maneuver by high-frequency oscillatory ventilation in experimental acute lung injury on organ blood flow in pigs
- PMID: 16836767
- PMCID: PMC1751024
- DOI: 10.1186/cc4967
Effect of a lung recruitment maneuver by high-frequency oscillatory ventilation in experimental acute lung injury on organ blood flow in pigs
Abstract
Introduction: The objective was to study the effects of a lung recruitment procedure by stepwise increases of mean airway pressure upon organ blood flow and hemodynamics during high-frequency oscillatory ventilation (HFOV) versus pressure-controlled ventilation (PCV) in experimental lung injury.
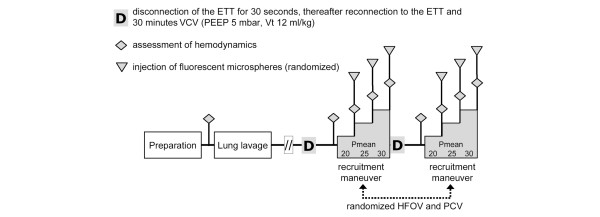
Methods: Lung damage was induced by repeated lung lavages in seven anesthetized pigs (23-26 kg). In randomized order, HFOV and PCV were performed with a fixed sequence of mean airway pressure increases (20, 25, and 30 mbar every 30 minutes). The transpulmonary pressure, systemic hemodynamics, intracranial pressure, cerebral perfusion pressure, organ blood flow (fluorescent microspheres), arterial and mixed venous blood gases, and calculated pulmonary shunt were determined at each mean airway pressure setting.
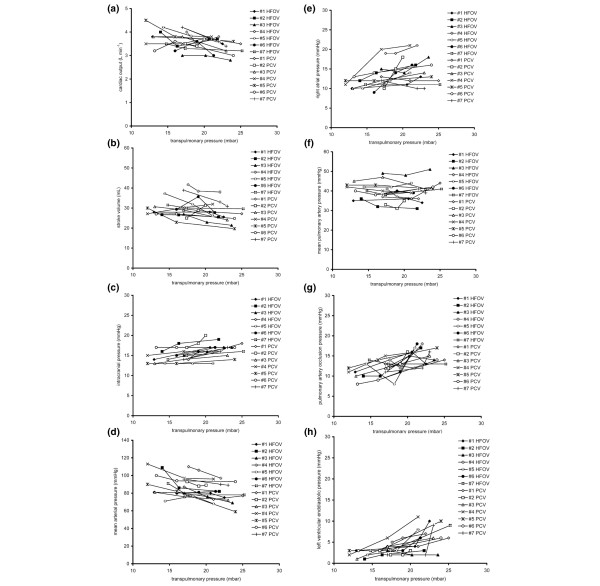
Results: The transpulmonary pressure increased during lung recruitment (HFOV, from 15 +/- 3 mbar to 22 +/- 2 mbar, P < 0.05; PCV, from 15 +/- 3 mbar to 23 +/- 2 mbar, P < 0.05), and high airway pressures resulted in elevated left ventricular end-diastolic pressure (HFOV, from 3 +/- 1 mmHg to 6 +/- 3 mmHg, P < 0.05; PCV, from 2 +/- 1 mmHg to 7 +/- 3 mmHg, P < 0.05), pulmonary artery occlusion pressure (HFOV, from 12 +/- 2 mmHg to 16 +/- 2 mmHg, P < 0.05; PCV, from 13 +/- 2 mmHg to 15 +/- 2 mmHg, P < 0.05), and intracranial pressure (HFOV, from 14 +/- 2 mmHg to 16 +/- 2 mmHg, P < 0.05; PCV, from 15 +/- 3 mmHg to 17 +/- 2 mmHg, P < 0.05). Simultaneously, the mean arterial pressure (HFOV, from 89 +/- 7 mmHg to 79 +/- 9 mmHg, P < 0.05; PCV, from 91 +/- 8 mmHg to 81 +/- 8 mmHg, P < 0.05), cardiac output (HFOV, from 3.9 +/- 0.4 l/minute to 3.5 +/- 0.3 l/minute, P < 0.05; PCV, from 3.8 +/- 0.6 l/minute to 3.4 +/- 0.3 l/minute, P < 0.05), and stroke volume (HFOV, from 32 +/- 7 ml to 28 +/- 5 ml, P < 0.05; PCV, from 31 +/- 2 ml to 26 +/- 4 ml, P < 0.05) decreased. Blood flows to the heart, brain, kidneys and jejunum were maintained. Oxygenation improved and the pulmonary shunt fraction decreased below 10% (HFOV, P < 0.05; PCV, P < 0.05). We detected no differences between HFOV and PCV at comparable transpulmonary pressures.
Conclusion: A typical recruitment procedure at the initiation of HFOV improved oxygenation but also decreased systemic hemodynamics at high transpulmonary pressures when no changes of vasoactive drugs and fluid management were performed. Blood flow to the organs was not affected during lung recruitment. These effects were independent of the ventilator mode applied.
Figures
Comment in
-
Ventilatory management of ARDS: high frequency oscillation and lung recruitment!Crit Care. 2006;10(4):158. doi: 10.1186/cc5018. Crit Care. 2006. PMID: 16934131 Free PMC article. Review.
-
Vital organ blood flow during high-frequency ventilation.Crit Care. 2006;10(6):426. doi: 10.1186/cc5075. Crit Care. 2006. PMID: 17118214 Free PMC article. No abstract available.
Similar articles
-
Alternative protocol to initiate high-frequency oscillatory ventilation: an experimental study.Crit Care. 2006;10(5):R138. doi: 10.1186/cc5052. Crit Care. 2006. PMID: 16999870 Free PMC article.
-
Sustained inflation and incremental mean airway pressure trial during conventional and high-frequency oscillatory ventilation in a large porcine model of acute respiratory distress syndrome.BMC Anesthesiol. 2006 Jun 22;6:8. doi: 10.1186/1471-2253-6-8. BMC Anesthesiol. 2006. PMID: 16792808 Free PMC article.
-
High-frequency oscillatory ventilation in experimental lung injury: effects on gas exchange.Intensive Care Med. 2002 Jun;28(6):768-74. doi: 10.1007/s00134-002-1288-4. Epub 2002 Apr 19. Intensive Care Med. 2002. PMID: 12107685
-
Reflections on pediatric high-frequency oscillatory ventilation from a physiologic perspective.Respir Care. 2012 Sep;57(9):1496-504. doi: 10.4187/respcare.01571. Epub 2012 Feb 17. Respir Care. 2012. PMID: 22348243 Review.
-
High frequency oscillatory ventilation in acute respiratory failure.Paediatr Respir Rev. 2004 Dec;5(4):323-32. doi: 10.1016/j.prrv.2004.07.002. Paediatr Respir Rev. 2004. PMID: 15531258 Review.
Cited by
-
Bench-to-bedside review: high-frequency oscillatory ventilation in adults with acute respiratory distress syndrome.Crit Care. 2006;10(6):240. doi: 10.1186/cc5096. Crit Care. 2006. PMID: 17184554 Free PMC article. Review.
-
High-frequency oscillatory ventilation and short-term outcome in neonates and infants undergoing cardiac surgery: a propensity score analysis.Crit Care. 2011;15(5):R259. doi: 10.1186/cc10521. Epub 2011 Oct 28. Crit Care. 2011. PMID: 22035562 Free PMC article.
-
Vital organ blood flow during high-frequency ventilation.Crit Care. 2006;10(6):426. doi: 10.1186/cc5075. Crit Care. 2006. PMID: 17118214 Free PMC article. No abstract available.
-
Year in review 2006: Critical Care--Respirology.Crit Care. 2007;11(4):224. doi: 10.1186/cc5963. Crit Care. 2007. PMID: 17764586 Free PMC article. Review.
-
Computed Tomography Assessment of Tidal Lung Overinflation in Domestic Cats Undergoing Pressure-Controlled Mechanical Ventilation During General Anesthesia.Front Vet Sci. 2022 Apr 1;9:842528. doi: 10.3389/fvets.2022.842528. eCollection 2022. Front Vet Sci. 2022. PMID: 35433898 Free PMC article.
References
-
- Derdak S, Mehta S, Stewart TE, Smith T, Rogers M, Buchman TG, Carlin B, Lowson S, Granton J, Multicenter Oscillatory Ventilation For Acute Respiratory Distress Syndrome Trial (MOAT) Study Investigators High-frequency oscillatory ventilation for acute respiratory distress syndrome in adults. Am J Respir Crit Care Med. 2002;166:801–808. doi: 10.1164/rccm.2108052. - DOI - PubMed
