

A multicenter randomized trial of computer-driven protocolized weaning from mechanical ventilation
- PMID: 16840741
- PMCID: PMC4788698
- DOI: 10.1164/rccm.200511-1780OC
A multicenter randomized trial of computer-driven protocolized weaning from mechanical ventilation
Abstract
Rationale and objectives: Duration of weaning from mechanical ventilation may be reduced by the use of a systematic approach. We assessed whether a closed-loop knowledge-based algorithm introduced in a ventilator to act as a computer-driven weaning protocol can improve patient outcomes as compared with usual care.
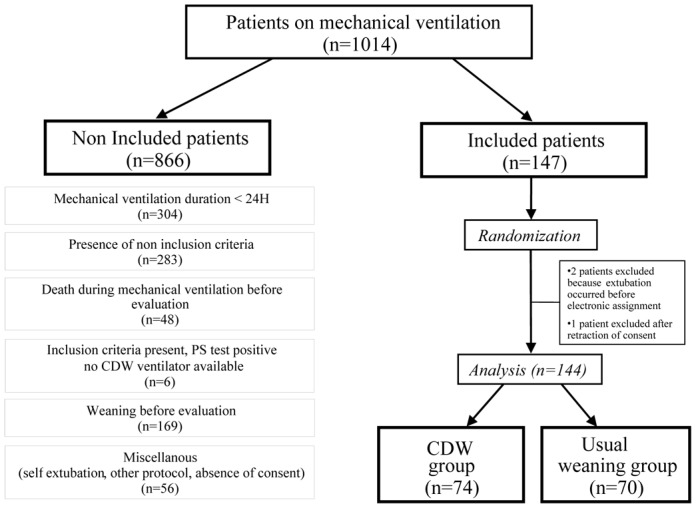
Methods and measurements: We conducted a multicenter randomized controlled study with concealed allocation to compare usual care for weaning with computer-driven weaning. The computerized protocol included an automatic gradual reduction in pressure support, automatic performance of spontaneous breathing trials (SBT), and generation of an incentive message when an SBT was successfully passed. One hundred forty-four patients were enrolled before weaning initiation. They were randomly allocated to computer-driven weaning or to physician-controlled weaning according to local guidelines. Weaning duration until successful extubation and total duration of ventilation were the primary endpoints.
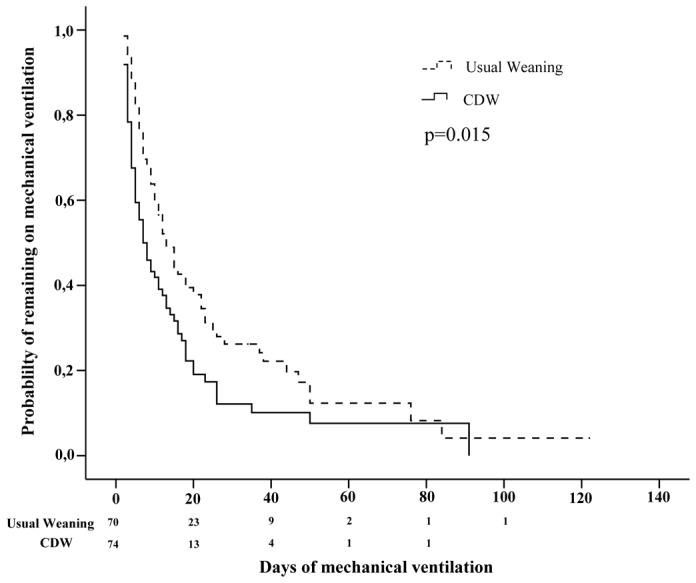
Main results: Weaning duration was reduced in the computer-driven group from a median of 5 to 3 d (p=0.01) and total duration of mechanical ventilation from 12 to 7.5 d (p=0.003). Reintubation rate did not differ (23 vs. 16%, p=0.40). Computer-driven weaning also decreased median intensive care unit (ICU) stay duration from 15.5 to 12 d (p=0.02) and caused no adverse events. The amount of sedation did not differ between groups. In the usual care group, compliance to recommended modes and to SBT was estimated, respectively, at 96 and 51%.
Conclusions: The specific computer-driven system used in this study can reduce mechanical ventilation duration and ICU length of stay, as compared with a physician-controlled weaning process.
Figures
Comment in
-
Just a spoonful of technology makes the protocol go down.Am J Respir Crit Care Med. 2006 Oct 15;174(8):849-51. doi: 10.1164/rccm.200607-933ED. Am J Respir Crit Care Med. 2006. PMID: 17021356 Free PMC article. No abstract available.
-
Computer-driven protocolized weaning from mechanical ventilation.Am J Respir Crit Care Med. 2007 May 1;175(9):968-9; author reply 969. doi: 10.1164/ajrccm.175.9.968. Am J Respir Crit Care Med. 2007. PMID: 17446346 No abstract available.
References
-
- Esteban A, Alia I, Ibanez J, Benito S, Tobin MJ. Modes of mechanical ventilation and weaning. A national survey of Spanish hospitals. The Spanish Lung Failure Collaborative Group. Chest. 1994;106:1188–93. - PubMed
-
- Esteban A, Anzueto A, Frutos F, Alia I, Brochard L, Stewart TE, Benito S, Epstein SK, Apezteguia C, Nightingale P, Arroliga AC, Tobin MJ. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. Jama. 2002;287:345–55. - PubMed
-
- Torres A, Aznar R, Gatell JM, Jimenez P, Gonzalez J, Ferrer A, Celis R, Rodriguez-Roisin R. Incidence, risk, and prognosis factors of nosocomial pneumonia in mechanically ventilated patients. Am Rev Respir Dis. 1990;142:523–8. - PubMed
-
- Fagon JY, Chastre J, Domart Y, Trouillet JL, Pierre J, Darne C, Gibert C. Nosocomial pneumonia in patients receiving continuous mechanical ventilation. Prospective analysis of 52 episodes with use of a protected specimen brush and quantitative culture techniques. Am Rev Respir Dis. 1989;139:877–84. - PubMed
-
- Epstein SK, Ciubotaru RL. Independent effects of etiology of failure and time to reintubation on outcome for patients failing extubation. Am J Respir Crit Care Med. 1998;158:489–93. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
