

Evaluation of a two-stage neural model of glaucomatous defect: an approach to reduce test-retest variability
- PMID: 16840874
- PMCID: PMC1808334
- DOI: 10.1097/01.opx.0000225091.60457.f4
Evaluation of a two-stage neural model of glaucomatous defect: an approach to reduce test-retest variability
Abstract
Purpose: The purpose of this study is to model perimetric defect and variability and identify stimulus conditions that can reduce variability while retaining good ability to detect glaucomatous defects.
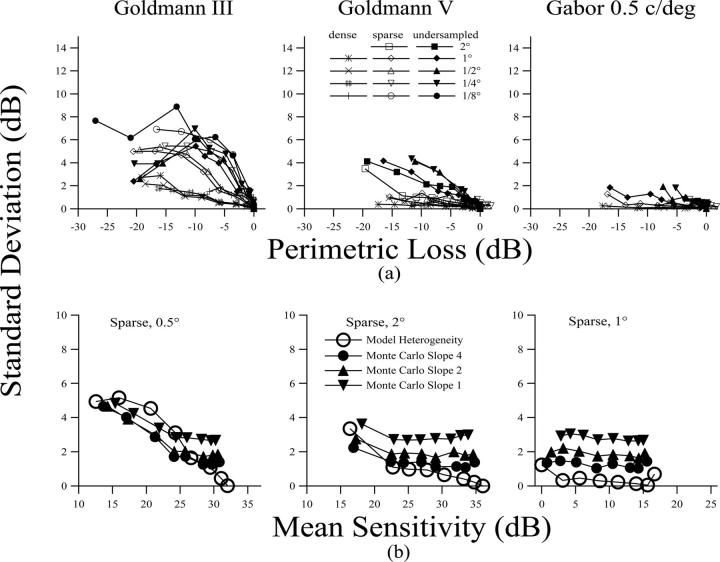
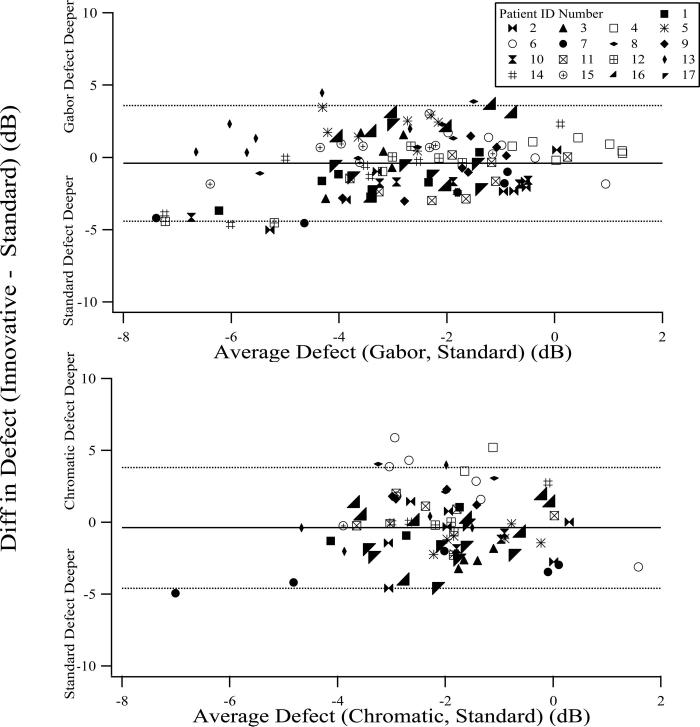
Methods: The two-stage neural model of Swanson et al. was extended to explore relations among perimetric defect, response variability, and heterogeneous glaucomatous ganglion cell damage. Predictions of the model were evaluated by testing patients with glaucoma using a standard luminance increment 0.43 degrees in diameter and two innovative stimuli designed to tap cortical mechanisms tuned to low spatial frequencies. The innovative stimuli were a luminance-modulated Gabor stimulus (0.5 c/deg) and circular equiluminant red-green chromatic stimuli whose sizes were close to normal Ricco's areas for the chromatic mechanism. Seventeen patients with glaucoma were each tested twice within a 2-week period. Sensitivities were measured at eight locations at eccentricities from 10 degrees to 21 degrees selected in terms of the retinal nerve fiber bundle patterns. Defect depth and response (test-retest) variability were compared for the innovative stimuli and the standard stimulus.
Results: The model predicted that response variability in defective areas would be lower for our innovative stimuli than for the conventional perimetric stimulus with similar defect depths if detection of the chromatic and Gabor stimuli was mediated by spatial mechanisms tuned to low spatial frequencies. Experimental data were consistent with these predictions. Depth of defect was similar for all three stimuli (F = 1.67, p > 0.19). Mean response variability was lower for the chromatic stimulus than for the other stimuli (F = 5.58, p < 0.005) and was lower for the Gabor stimulus than for the standard stimulus in areas with more severe defects (t = 2.68, p < 0.005). Variability increased with defect depth for the standard and Gabor stimuli (p < 0.005) but not for the chromatic stimulus (slope less than zero).
Conclusions: Use of large perimetric stimuli detected by cortical mechanisms tuned to low spatial frequencies can make it possible to lower response variability without comprising the ability to detect glaucomatous defect.
Figures






References
-
- Swanson WH, Felius J, Pan F. Perimetric defects and ganglion cell damage: interpreting linear relations using a two-stage neural model. Invest Ophthalmol Vis Sci. 2004;45:466–72. - PubMed
-
- Coleman AL. Glaucoma. Lancet. 1999;354:1803–10. - PubMed
-
- Heijl A, Lindgren A, Lindgren G. Test-retest variability in glaucomatous visual fields. Am J Ophthalmol. 1989;108:130–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
