

Effect of rhPDGF-BB delivery on mediators of periodontal wound repair
- PMID: 16846342
- PMCID: PMC2586965
- DOI: 10.1089/ten.2006.12.1441
Effect of rhPDGF-BB delivery on mediators of periodontal wound repair
Abstract
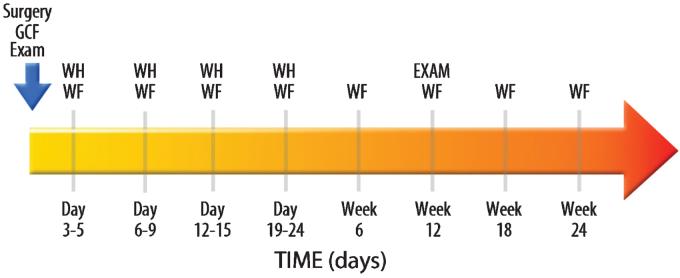
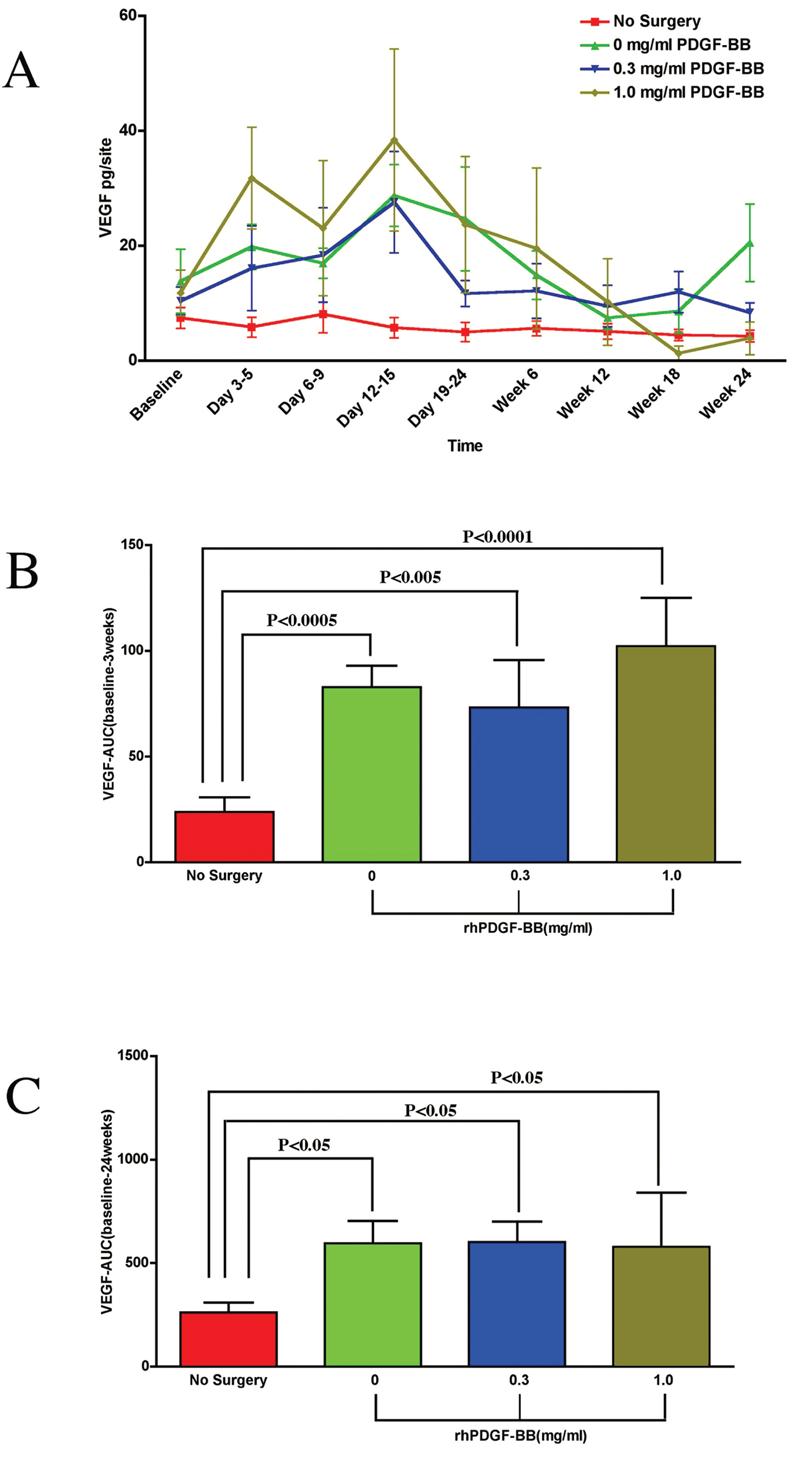
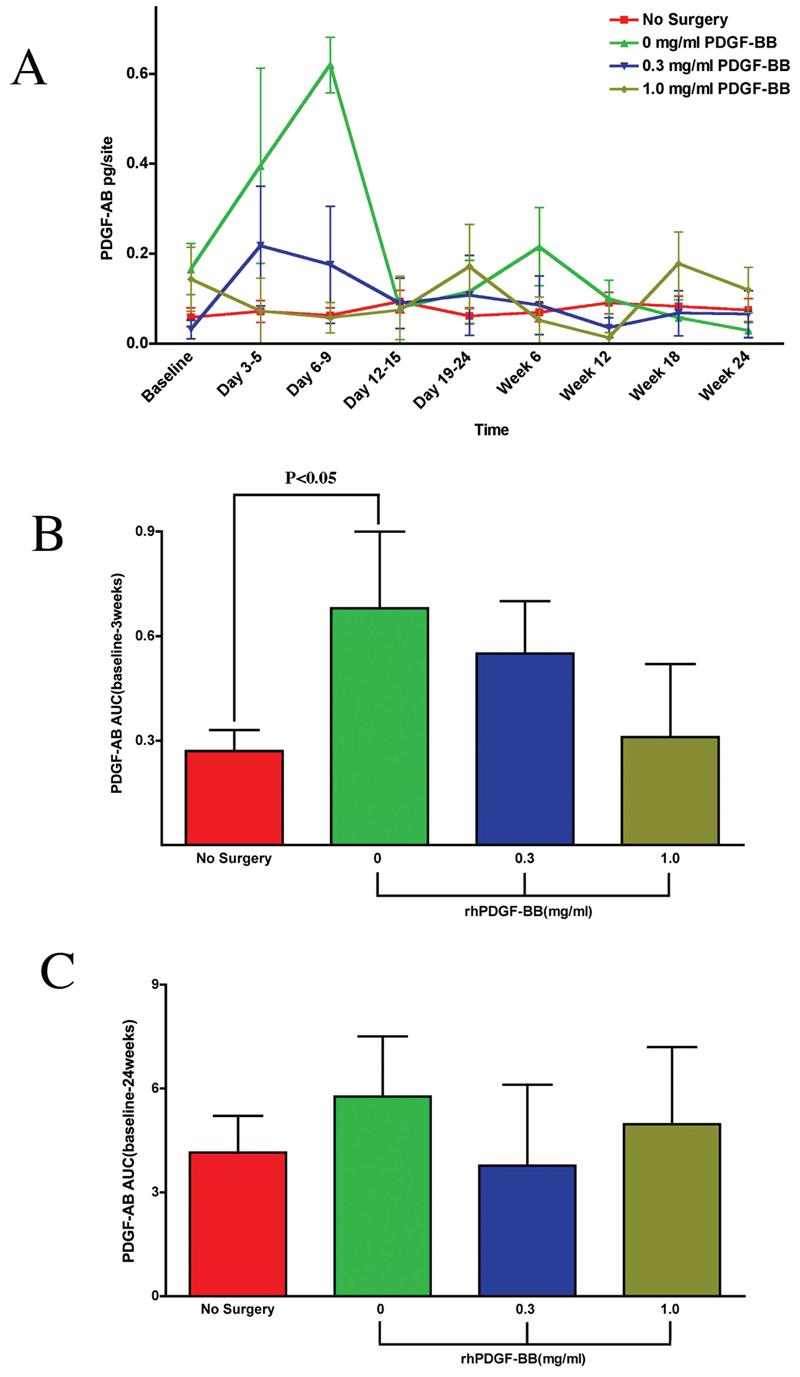
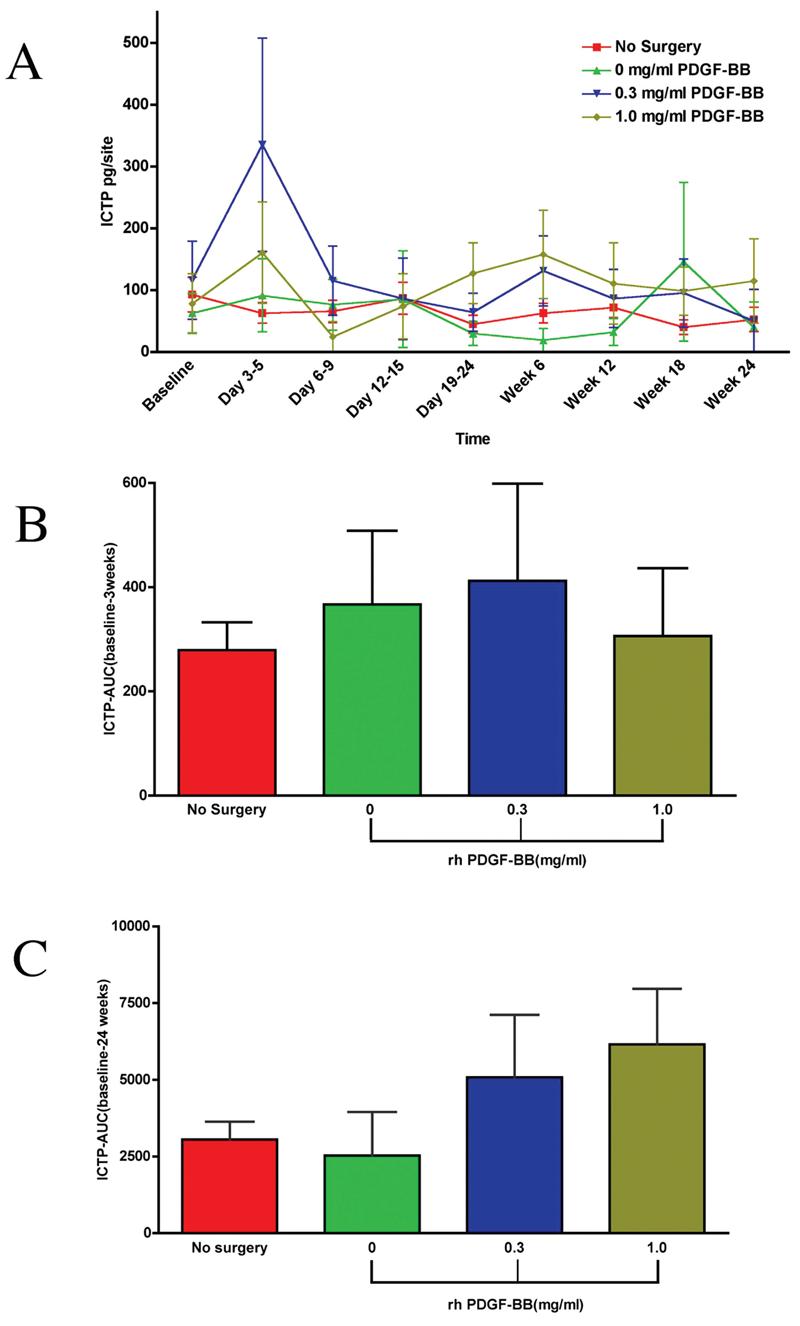
Growth factors such as platelet-derived growth factor (PDGF) exert potent effects on wound healing including the regeneration of tooth-supporting structures. This investigation examined the effect of the local delivery of PDGF-BB when combined with reconstructive periodontal surgery on local wound fluid (WF) levels of PDGF-AB, vascular endothelial growth factor (VEGF), and bone collagen telopeptide (ICTP) in humans with advanced periodontitis. Sixteen patients exhibiting localized periodontal osseous defects were randomized to one of three groups (beta-TCP carrier alone, beta-TCP + 0.3 mg/mL of recombinant human PDGF-BB [rhPDGF-BB], or beta-TCP + 1.0 mg/mL of rhPDGF-BB) and monitored for 6 months. WF was harvested and analyzed for PDGF-AB, VEGF, and ICTP WF levels. Teeth contralateral to the target lesions served as controls. Increased levels of VEGF in the WF was observed for all surgical treatment groups with the 1.0 mg/mL rhPDGF-BB group showing the most pronounced difference at 3 weeks in the AUC analysis versus control (p < 0.0001). PDGF-AB WF levels were increased for the carrier alone group compared to both rhPDGFBB groups. Low-dose rhPDGF-BB application elicited increases in ICTP at days 3-5 in the wound healing process, suggesting a promotion of bone turnover at early stages of the repair process (p < 0.02). These results demonstrate contrasting inducible expression patterns of PDGF-AB, VEGF, and ICTP during periodontal wound healing in humans.
Figures
References
-
- Williams RC. Periodontal disease. N. Engl. J. Med. 1990;322:373. - PubMed
-
- Heldin CH. Platelet-derived growth factor—an introduction. Cytokine Growth Factor Rev. 2004;15:195. - PubMed
-
- Heldin CH, Ostman A, Ronnstrand L. Signal transduction via platelet-derived growth factor receptors. Biochim. Biophys. Acta. 1998;1378:F79. - PubMed
-
- Rosenkranz S, Kazlauskas A. Evidence for distinct signaling properties and biological responses induced by the PDGF receptor alpha and beta subtypes. Growth Factors. 1999;16:201. - PubMed
-
- Lynch SE, de Castilla GR, Williams RC, Kiritsy CP, Howell TH, Reddy MS, Antoniades HN. The effects of short-term application of a combination of platelet-derived and insulin-like growth factors on periodontal wound healing. J. Periodontol. 1991;62:458. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
