

Magnetocardiographic assessment of healed myocardial infarction
- PMID: 16846435
- PMCID: PMC6932496
- DOI: 10.1111/j.1542-474X.2006.00106.x
Magnetocardiographic assessment of healed myocardial infarction
Abstract
Background: We evaluated the capability of multichannel magnetocardiography (MCG) to detect healed myocardial infarction (MI).
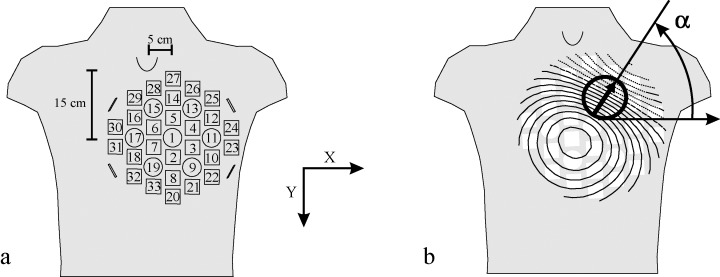
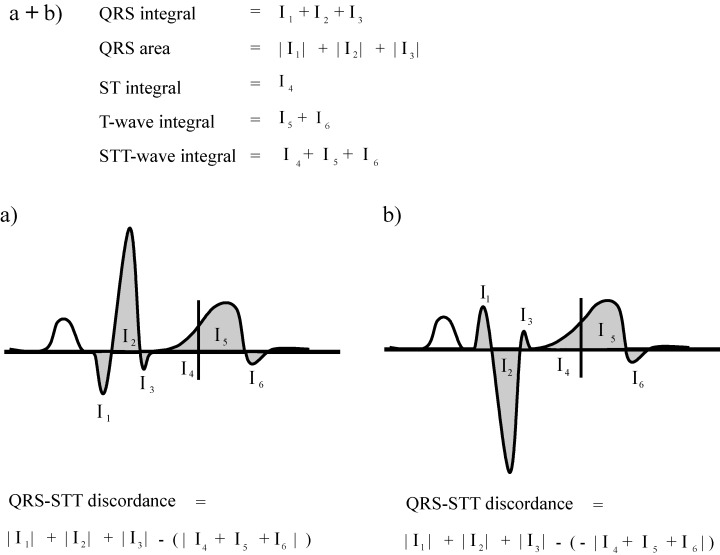
Methods: Multichannel MCG over frontal chest was recorded at rest in 21 patients with healed MI, detected by cine- and contrast-enhanced magnetic resonance imaging, and in 26 healthy controls. Of the 21 MI patients, 11 had non-Q wave and 10 Q wave MIs. QRS, ST-segment, T wave and ST-T wave integrals, ST-segment and T wave amplitudes, and QRS and ST-T wave magnetic field map orientations were measured.
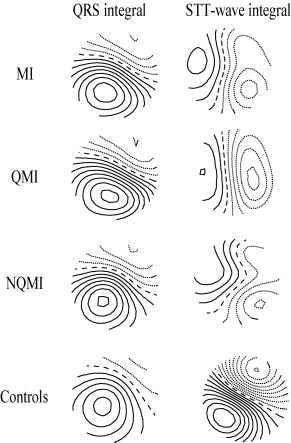
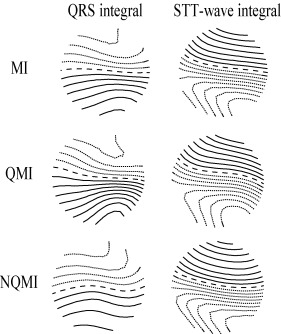
Results: The MCG repolarization indexes, such as ST segment and ST-T wave integrals, separated the MI group from the controls (ST-T wave integral -1.4 +/- 5.3 vs 1.5 +/- 4.7 pTs, P = 0.034). The abnormalities were more distinct in the Q wave-MI than in the non-Q wave MI subgroup. In the latter, however, a trend similar to the Q wave MI group was found. The relation of QRS area to ST segment and T wave integral improved the detection of healed MIs compared to the ST-T wave indexes alone (QRS-ST-T discordance 14 +/- 10 vs 5.0 +/- 7.1 pTs, P = 0.003). When comparing the MI group to the controls, the orientation of the magnetic field maps differed in the ST-T wave maps (163 +/- 119 degrees vs 58 +/- 17 degrees, P < 0.001) but not in the QRS maps (111 +/- 95 degrees vs 106 +/-93 degrees, P = 0.646).
Conclusions: The MCG repolarization variables can detect healed MI. These ST-T wave abnormalities are more pronounced in patients with Q wave MI than in patients with non-Q wave MIs. Relating the signals of depolarization and repolarization phases improves the detection of healed MI. Repolarization abnormalities are common in healed MI and thus should not always be interpreted as present ongoing ischemia.
Figures
References
-
- Bertrand ME, Simoons ML, Fox KAA, et al Management of acute coronary syndromes in patients presenting without persistent ST‐segment elevation. Eur Heart J 2002;23:1809–1840. - PubMed
-
- Siltanen P. Magnetocardiography In MacFarlane P. (ed.): Comprehensive Electrocardiology, Vol. II New York , Pergamon Press, 1989, pp. 1408–1438.
-
- Nenonen J, Montonen J, Mäkijärvi M. Principles of magnetocardiographic mapping In Shenasa M, Borgreffe M, Breithardt G. (eds.): Cardiac Mapping, 2nd Edition Mount Kisco , NY , Futura Publishing Co., 2002, pp. 119–130.
-
- Brockmeier K, Schmitz L, Chavez JJB, et al Magnetocardiography and 32‐lead potential mapping: Repolarization in normal subjects during pharmacologically induced stress. J Cardiovasc Electrophysiol 1997;8:615–626. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
