

A radial basis classifier for the automatic detection of aspiration in children with dysphagia
- PMID: 16846507
- PMCID: PMC1570357
- DOI: 10.1186/1743-0003-3-14
A radial basis classifier for the automatic detection of aspiration in children with dysphagia
Abstract
Background: Silent aspiration or the inhalation of foodstuffs without overt physiological signs presents a serious health issue for children with dysphagia. To date, there are no reliable means of detecting aspiration in the home or community. An assistive technology that performs in these environments could inform caregivers of adverse events and potentially reduce the morbidity and anxiety of the feeding experience for the child and caregiver, respectively. This paper proposes a classifier for automatic classification of aspiration and swallow vibration signals non-invasively recorded on the neck of children with dysphagia.
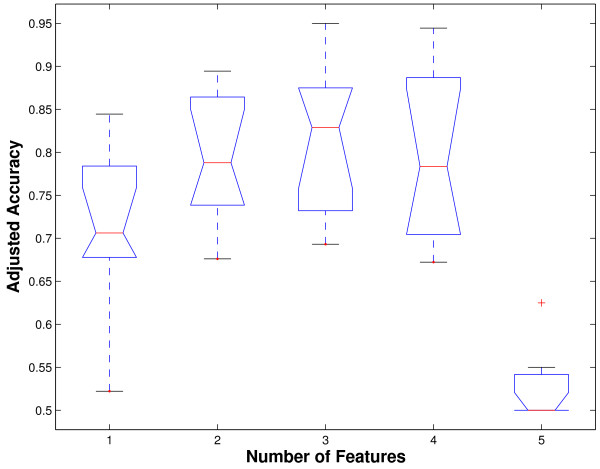
Methods: Vibration signals associated with safe swallows and aspirations, both identified via videofluoroscopy, were collected from over 100 children with neurologically-based dysphagia using a single-axis accelerometer. Five potentially discriminatory mathematical features were extracted from the accelerometry signals. All possible combinations of the five features were investigated in the design of radial basis function classifiers. Performance of different classifiers was compared and the best feature sets were identified.
Results: Optimal feature combinations for two, three and four features resulted in statistically comparable adjusted accuracies with a radial basis classifier. In particular, the feature pairing of dispersion ratio and normality achieved an adjusted accuracy of 79.8 +/- 7.3%, a sensitivity of 79.4 +/- 11.7% and specificity of 80.3 +/- 12.8% for aspiration detection. Addition of a third feature, namely energy, increased adjusted accuracy to 81.3 +/- 8.5% but the change was not statistically significant. A closer look at normality and dispersion ratio features suggest leptokurticity and the frequency and magnitude of atypical values as distinguishing characteristics between swallows and aspirations. The achieved accuracies are 30% higher than those reported for bedside cervical auscultation.
Conclusion: The proposed aspiration classification algorithm provides promising accuracy for aspiration detection in children. The classifier is conducive to hardware implementation as a non-invasive, portable "aspirometer". Future research should focus on further enhancement of accuracy rates by considering other signal features, classifier methods, or an augmented variety of training samples. The present study is an important first step towards the eventual development of wearable intelligent intervention systems for the diagnosis and management of aspiration.
Figures






Similar articles
-
A radial basis function classifier for pediatric aspiration detection.Conf Proc IEEE Eng Med Biol Soc. 2006;2006:3553-6. doi: 10.1109/IEMBS.2006.260343. Conf Proc IEEE Eng Med Biol Soc. 2006. PMID: 17945784
-
Automatic discrimination between safe and unsafe swallowing using a reputation-based classifier.Biomed Eng Online. 2011 Nov 15;10:100. doi: 10.1186/1475-925X-10-100. Biomed Eng Online. 2011. PMID: 22085802 Free PMC article.
-
A Preliminary Investigation of Similarities of High Resolution Cervical Auscultation Signals Between Thin Liquid Barium and Water Swallows.IEEE J Transl Eng Health Med. 2021 Dec 10;10:4900109. doi: 10.1109/JTEHM.2021.3134926. eCollection 2022. IEEE J Transl Eng Health Med. 2021. PMID: 34963825 Free PMC article.
-
Early assessments of dysphagia and aspiration risk in acute stroke patients.Stroke. 2003 May;34(5):1252-7. doi: 10.1161/01.STR.0000066309.06490.B8. Epub 2003 Apr 3. Stroke. 2003. PMID: 12677020 Review.
-
Creating robust, reliable, clinically relevant classifiers from spectroscopic data.Biophys Rev. 2009 Dec;1(4):201-211. doi: 10.1007/s12551-009-0023-6. Epub 2009 Nov 25. Biophys Rev. 2009. PMID: 28510028 Free PMC article. Review.
Cited by
-
Computer-aided screening of aspiration risks in dysphagia with wearable technology: a Systematic Review and meta-analysis on test accuracy.Front Bioeng Biotechnol. 2023 Jun 27;11:1205009. doi: 10.3389/fbioe.2023.1205009. eCollection 2023. Front Bioeng Biotechnol. 2023. PMID: 37441197 Free PMC article.
-
Characteristics of the swallowing sounds recorded in the ear, nose and on trachea.Med Biol Eng Comput. 2012 Aug;50(8):885-90. doi: 10.1007/s11517-012-0938-0. Epub 2012 Jul 18. Med Biol Eng Comput. 2012. PMID: 22802141
-
Effects of liquid stimuli on dual-axis swallowing accelerometry signals in a healthy population.Biomed Eng Online. 2010 Feb 4;9:7. doi: 10.1186/1475-925X-9-7. Biomed Eng Online. 2010. PMID: 20128928 Free PMC article.
-
Deep Learning for Classification of Normal Swallows in Adults.Neurocomputing (Amst). 2018 Apr 12;285:1-9. doi: 10.1016/j.neucom.2017.12.059. Epub 2018 Jan 31. Neurocomputing (Amst). 2018. PMID: 29755210 Free PMC article.
-
Detection of swallows with silent aspiration using swallowing and breath sound analysis.Med Biol Eng Comput. 2012 Dec;50(12):1261-8. doi: 10.1007/s11517-012-0958-9. Epub 2012 Oct 13. Med Biol Eng Comput. 2012. PMID: 23065649
References
-
- Groher M, Gonzalez E. Mechanical disorders of swallowing. In: Groher M, editor. Dysphagia: diagnosis and management. Stoneham, MA: Butterworth-Heinemann; 1992. pp. 53–84.
-
- Sheppard J. Pediatric dysphagia and related medical, behavioral and developmental issues. In: Sonies B, editor. Dysphagia: a continuum of care. Gaithersburg, MD: Aspen Publishers Inc; 1997. pp. 55–74.
-
- Doty R. Neural organization of deglutition. In: Code C, editor. Handbook of physiology: alimenatray canal motility. Washington, DC: American Physiological Society; 1998. pp. 1861–1902.
-
- Zorowitz R, Robinson K. Pathophysiology of dysphagia and aspiration. Topics in Stroke Rehabilitation. 1999;6:1–16. doi: 10.1310/LT3H-H5UF-F6V9-6KK8. - DOI
-
- Logemann J. Evaluation and treatment of swallowing disorders. Austin, TX: Pro Ed; 1997.
LinkOut - more resources
Full Text Sources
Other Literature Sources
