

Comparison of laparoscopic and mini incision open donor nephrectomy: single blind, randomised controlled clinical trial
- PMID: 16847014
- PMCID: PMC1523437
- DOI: 10.1136/bmj.38886.618947.7C
Comparison of laparoscopic and mini incision open donor nephrectomy: single blind, randomised controlled clinical trial
Abstract
Objectives: To determine the best approach for live donor nephrectomy to minimise discomfort to the donor and to provide good graft function.
Design: Single blind, randomised controlled trial.
Setting: Two university medical centres, the Netherlands.
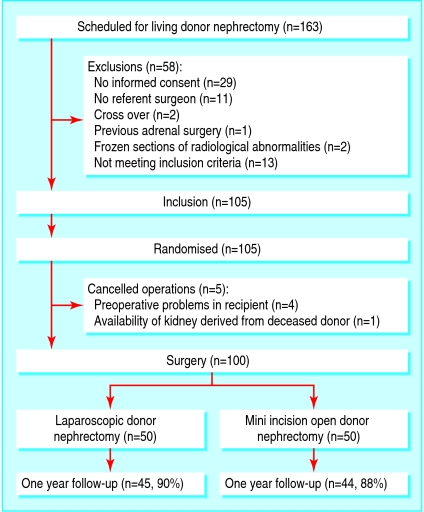
Participants: 100 living kidney donors.
Interventions: Participants were randomly assigned to either laparoscopic donor nephrectomy or to mini incision muscle splitting open donor nephrectomy.
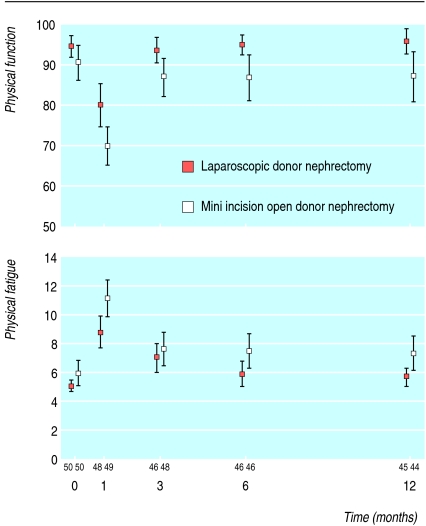
Main outcome measures: The primary outcome was physical fatigue using the multidimensional fatigue inventory 20 (MFI-20). Secondary outcomes were physical function using the SF-36, hospital stay after surgery, pain, operating times, recipient graft function, and graft survival.
Results: Conversions did not occur. Compared with mini incision open donor nephrectomy, laparoscopic donor nephrectomy resulted in longer skin to skin time (median 221 v 164 minutes, P < 0.001), longer warm ischaemia time (6 v 3 minutes, P < 0.001), less blood loss (100 v 240 ml, P < 0.001), and a similar number of complications (intraoperatively 12% v 6%, P = 0.49, postoperatively both 6%). After laparoscopic nephrectomy, donors required less morphine (16 v 25 mg, P = 0.005) and shorter hospital stay (3 v 4 days, P = 0.003). During one year's follow-up mean physical fatigue was less (difference - 1.3, 95% confidence interval - 2.4 to - 0.1) and physical function was better (difference 6.2, 2.0 to 10.3) after laparoscopic nephrectomy. Function of the graft and graft survival rate of the recipient at one year censored for death did not differ (100% after laparoscopic nephrectomy and 98% after open nephrectomy).
Conclusions: Laparoscopic donor nephrectomy results in a better quality of life compared with mini incision open donor nephrectomy but equal safety and graft function.
Figures
Republished in
-
[Donor nephrectomy: less fatigue and better quality of life following laparoscopic kidney removal compared with an open procedure by mini-incision: blind randomised study].Ned Tijdschr Geneeskd. 2007 Jun 16;151(24):1352-60. Ned Tijdschr Geneeskd. 2007. PMID: 17665628 Dutch.
Comment in
-
Quality of life after donor nephrectomy.BMJ. 2006 Jul 29;333(7561):209-10. doi: 10.1136/bmj.333.7561.209. BMJ. 2006. PMID: 16873832 Free PMC article. No abstract available.
-
Is laparoscopic donor nephrectomy the new standard?Nat Clin Pract Urol. 2007 Apr;4(4):186-7. doi: 10.1038/ncpuro0755. Epub 2007 Mar 6. Nat Clin Pract Urol. 2007. PMID: 17342098 No abstract available.
References
-
- Ingelfinger JR. Risks and benefits to the living donor. N Engl J Med 2005;353: 447-9. - PubMed
-
- Ratner LE, Ciseck LJ, Moore RG, Cigarroa FG, Kaufman HS, Kavoussi LR. Laparoscopic live donor nephrectomy. Transplantation 1995;60: 1047-9. - PubMed
-
- Srivastava A, Tripathi DM, Zaman W, Kumar A. Subcostal versus transcostal mini donor nephrectomy: is rib resection responsible for pain related donor morbidity. J Urol 2003;170: 738-40. - PubMed
-
- Yang SL, Harkaway R, Badosa F, Ginsberg P, Greenstein MA. Minimal incision living donor nephrectomy: improvement in patient outcome. Urology 2002;59: 673-7. - PubMed
-
- Kok NF, Alwayn IP, Lind MY, Tran KT, Weimar W, Ijzermans JN. Donor nephrectomy: mini-incision muscle-splitting open approach versus laparoscopy. Transplantation 2006;81: 881-7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical