

'SOSORT consensus paper on brace action: TLSO biomechanics of correction (investigating the rationale for force vector selection)'
- PMID: 16857045
- PMCID: PMC1553475
- DOI: 10.1186/1748-7161-1-11
'SOSORT consensus paper on brace action: TLSO biomechanics of correction (investigating the rationale for force vector selection)'
Abstract
Background: The effectiveness of orthotic treatment continues to be controversial in international medical literature due to differences in the reported results and conclusions of various studies. Heterogeneity of the samples has been suggested as a reason for conflicting results. Besides the obvious theoretical differences between the brace concepts, the variability in the technical factors can also explain the contradictory results between same brace types. This paper will investigate the degree of variability among responses of scoliosis specialists from the Brace Study Ground of the International Society on Scoliosis Orthopedic and Rehabilitation Treatment SOSORT. Ultimately, this information could be a foundation for establishing a consensus and framework for future prospective controlled studies.
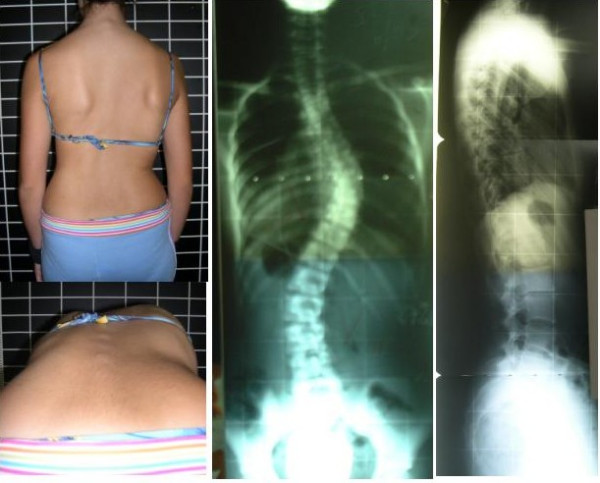
Methods: A preliminary questionnaire on the topic of 'brace action' relative to the theory of three-dimensional scoliosis correction and brace treatment was developed and circulated to specialists interested in the conservative treatment of adolescent idiopathic scoliosis. A particular case was presented (main thoracic curve with minor lumbar). Several key points emerged and were used to develop a second questionnaire which was discussed and full filed after the SOSORT consensus meeting (Milano, Italy, January 2005).
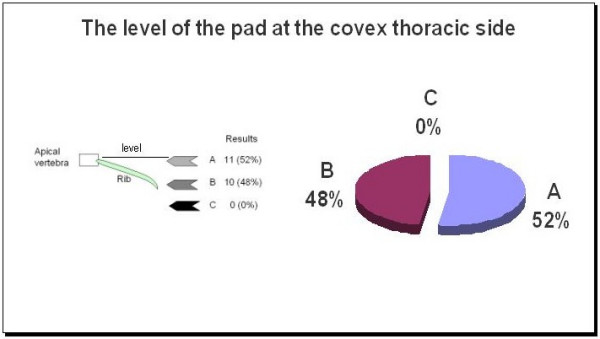
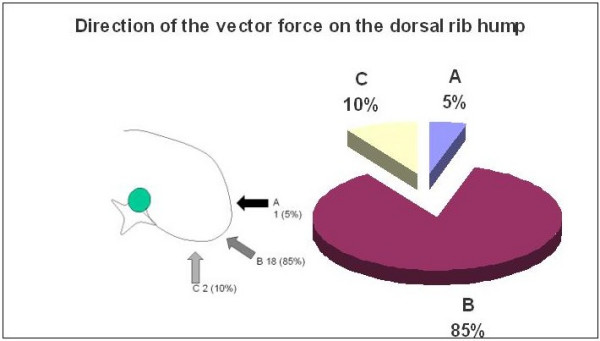
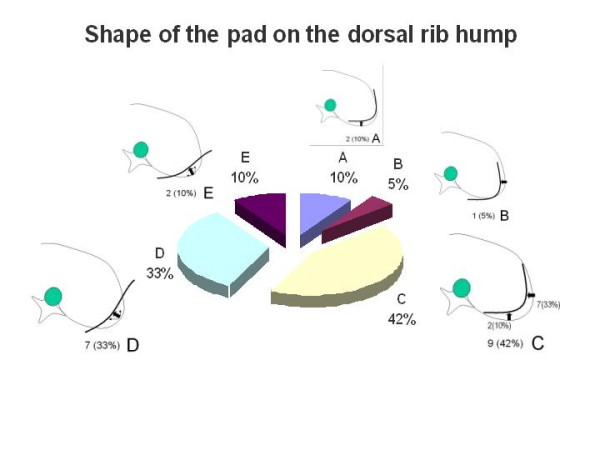
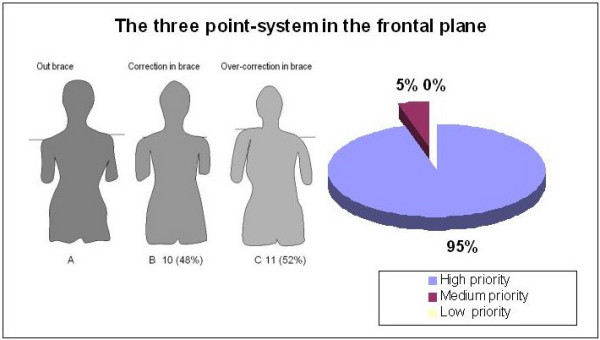
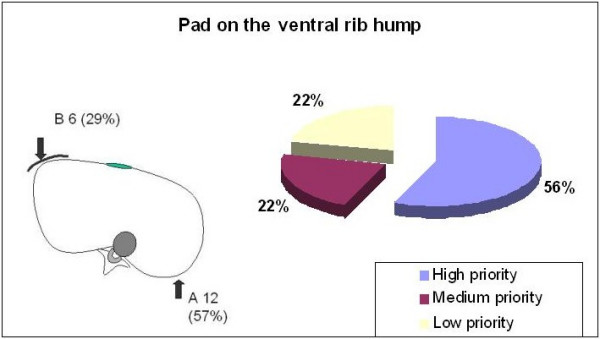
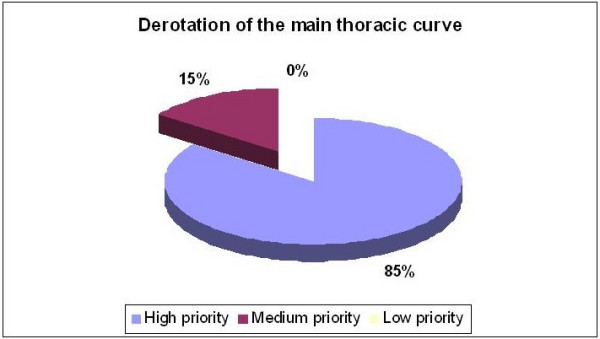
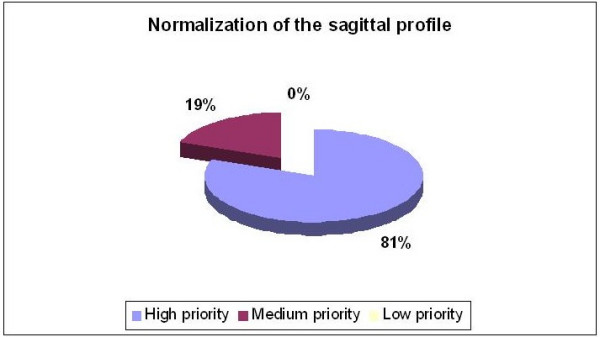
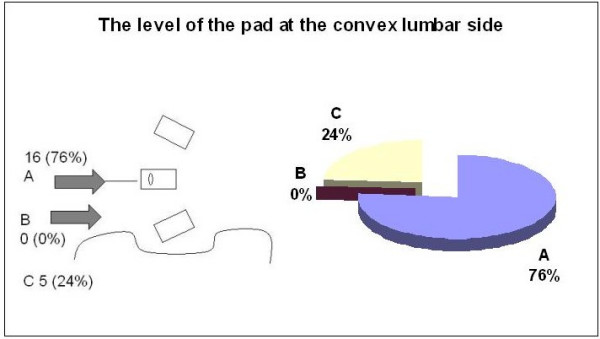
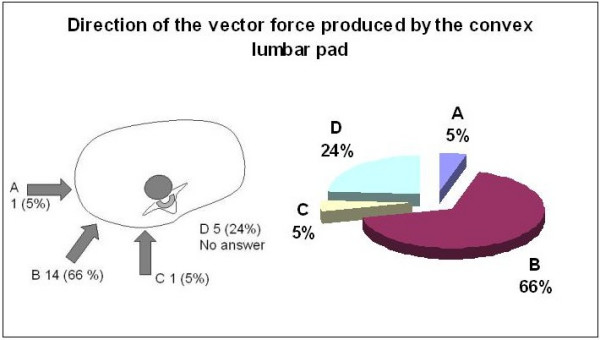
Results: Twenty-one questionnaires were completed. The Chêneau brace was the most frequently recommended. The importance of the three point system mechanism was stressed. Options about proper pad placement on the thoracic convexity were divided 50% for the pad reaching or involving the apical vertebra and 50% for the pad acting caudal to the apical vertebra. There was agreement about the direction of the vector force, 85% selecting a 'dorso lateral to ventro medial' direction but about the shape of the pad to produce such a force. Principles related to three-dimensional correction achieved high consensus (80%-85%), but suggested methods of correction were quite diverse.
Conclusion: This study reveals that among participating SOSORT specialists there continues to be a strongly held and conflicting if not a contentious opinion regarding brace design and treatment. If the goal of a 'treatment consensus' is realistic and achievable, significantly more effort will be required to reconcile these differences.
Figures
References
-
- Noonan KJ, Weinstein SL, Jacobson WC, Dolan LA. Use of the Milwaukee brace for progressive idiopathic scoliosis. J Bone Joint Surg Am. 1996;78:557–567. - PubMed
-
- Goldberg CJ, Fogarty EE, Hal JE, Emans JB. A statistical comparison between natural history of idiopathic scoliosis and brace treatment in skeletally immature adolescent girls. Spine. 1993;18:902–908. - PubMed
-
- Nachemson AL, Peterson LE, Members of the brace study group of the Scoliosis Research Society Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. A prospective, controlled study based on data from the brace study of the SRS. J Bone Joint Surg Am. 1995;77:815–822. - PubMed
-
- Weiss HR, Weiss G, Schaar H. Conservative management in patients with scoliosis: does it reduce the incidence of surgery? In: Grivas Th, editor. proceedings of the International Research Society of Spinal Deformities: 24–27 May 2002; Athens. 2002. p. 84. - PubMed
