

Risk factors for long-term pain after hernia surgery
- PMID: 16858183
- PMCID: PMC1602172
- DOI: 10.1097/01.sla.0000218081.53940.01
Risk factors for long-term pain after hernia surgery
Abstract
Objective: To estimate the prevalence of residual pain 2 to 3 years after hernia surgery, to identify factors associated with its occurrence, and to assess the consequences for the patient.
Summary background data: Iatrogenic chronic pain is a neglected problem that may totally annul the benefits from hernia repair.
Methods: From the population-based Swedish Hernia Register 3000 patients aged 15 to 85 years were sampled from the 9280 patients registered as having undergone a primary groin hernia operation in the year 2000. Of these, the 2853 patients still alive in 2003 were requested to fill in a postal questionnaire.
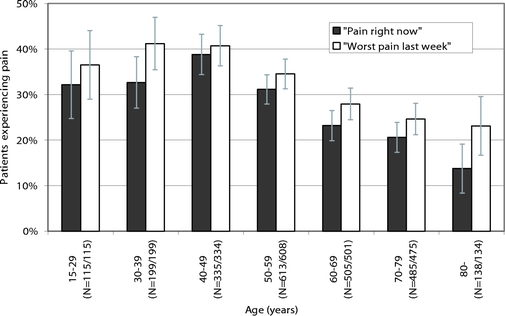
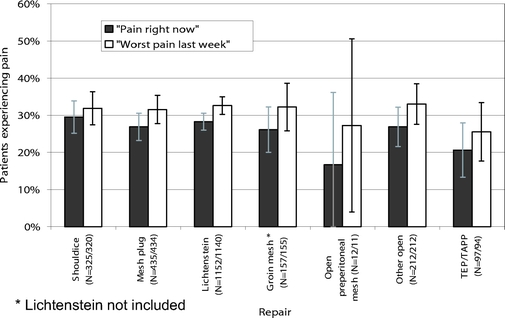
Results: After 2 reminders, 2456 patients (86%), 2299 men and 157 women responded. In response to a question about "worst perceived pain last week," 758 patients (31%) reported pain to some extent. In 144 cases (6%), the pain interfered with daily activities. Age below median, a high level of pain before the operation, and occurrence of any postoperative complication were found to significantly and independently predict long-term pain in multivariate logistic analysis when "worst pain last week" was used as outcome variable. The same variables, along with a repair technique using anterior approach, were found to predict long-term pain with "pain right now" as outcome variable.
Conclusion: Pain that is at least partly disabling appears to occur more often than recurrences. The prevalence of long-term pain can be reduced by preventing postoperative complications. The impact of repair technique on the risk of long-term pain shown in our study should be further assessed in randomized controlled trials.
Figures
References
-
- Nilsson E, Haapaniemi S. Hernia registers and specialization. Surg Clin North Am. 1998;78:1141–1155. - PubMed
-
- Kehlet H, Bay-Nielsen M, Kingsnorth A. Chronic postherniorrhaphy pain: a call for uniform assessment. Hernia. 2002;6:178–181. - PubMed
-
- SBR (Swedish Hernia Register web site). May 8, 2005. Available at https://sbr.norrnod.se/html/welcome.stm.
-
- Franneby U, Gunnarsson U, Wollert S, et al. Discordance between the patient's and surgeon's perception of complications following hernia surgery. Hernia. 2005;9:145–149. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
