

An uncommon cause of paraplegia: Salmonella spondylodiskitis
- PMID: 16859227
- PMCID: PMC1864813
- DOI: 10.1080/10790268.2006.11753879
An uncommon cause of paraplegia: Salmonella spondylodiskitis
Abstract
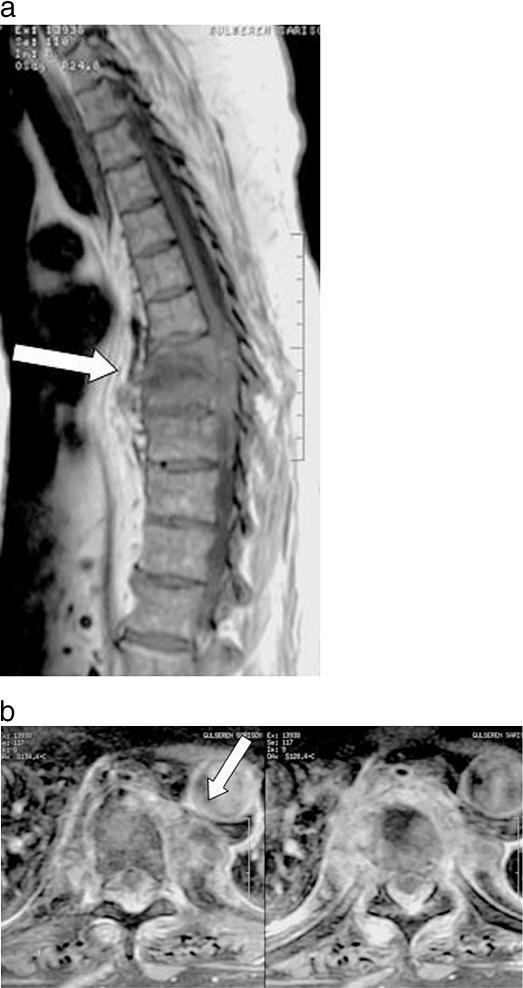
Background/objective: Salmonella spondylodiskitis is an uncommon type of vertebral infection. The aim of this study was to present a case of progressive paraplegia caused by Salmonella spondylodiskitis and epidural abscess after endoscopic cholecystectomy.
Methods: The patient underwent posterior instrumentation and posterior fusion between T6 and T12, hemilaminotomies at levels T8-T9-T10, and drainage of the abscess. Through a left thoracotomy, anterior T8-T10 corpectomy, debridement, anterior stabilization, and fusion were conducted.
Results: Fifteen months later, final follow-up showed no complications secondary to the vertebral and hip surgeries, and neurological status improved to Frankel grade E. Laboratory investigations showed no evidence of Salmonella infection.
Conclusion: Immunocompromised patients who undergo endoscopic intervention are vulnerable to Salmonella infections. One must consider Salmonella infection in those who develop acute progressive spondylodiskitis.
Figures

Similar articles
-
Complete recovery of acute paraplegia due to pyogenic thoracic spondylodiscitis with an epidural abscess.Acta Neurochir (Wien). 2008 Apr;150(4):381-6. doi: 10.1007/s00701-007-1485-6. Epub 2008 Jan 8. Acta Neurochir (Wien). 2008. PMID: 18176773
-
Epidural abscess as a delayed complication of spinal instrumentation in scoliosis surgery: a case of progressive neurologic dysfunction with complete recovery.Spine (Phila Pa 1976). 2008 Feb 1;33(3):E76-80. doi: 10.1097/BRS.0b013e31816245a6. Spine (Phila Pa 1976). 2008. PMID: 18303449
-
Posterior fixation without debridement for vertebral body osteomyelitis and discitis.Neurosurg Focus. 2014 Aug;37(2):E6. doi: 10.3171/2014.6.FOCUS14142. Neurosurg Focus. 2014. PMID: 25081966
-
Spontaneous corynebacterium spondylodiskitis in an immunocompetent patient: A case report and literature review.J Spinal Cord Med. 2016 Nov;39(6):730-733. doi: 10.1179/2045772315Y.0000000040. Epub 2015 Jun 25. J Spinal Cord Med. 2016. PMID: 26111121 Free PMC article. Review.
-
Candida spondylodiscitis and epidural abscess: management with shorter courses of anti-fungal therapy in combination with surgical debridement.J Infect. 2005 Jul;51(1):17-23. doi: 10.1016/j.jinf.2004.08.020. J Infect. 2005. PMID: 15979485 Review.
Cited by
-
Spine Infections: The Role of Fluorodeoxyglucose Positron Emission Tomography (FDG PET) in the Context of the Actual Diagnosis Guideline.Curr Med Imaging. 2022;18(2):216-230. doi: 10.2174/1573405617666210916121046. Curr Med Imaging. 2022. PMID: 34530718 Free PMC article. Review.
-
A case of canine discospondylitis and epidural empyema due to Salmonella species.Can Vet J. 2013 Jun;54(6):595-8. Can Vet J. 2013. PMID: 24155452 Free PMC article.
-
Gallbladder Empyema and Epidural Abscess Due to Salmonella Enteritidis After Treatment of Primary Infection: Case Report and Review of the Literature.Open Forum Infect Dis. 2023 Aug 12;10(8):ofad432. doi: 10.1093/ofid/ofad432. eCollection 2023 Aug. Open Forum Infect Dis. 2023. PMID: 37608918 Free PMC article.
-
Salmonella potsdam causing lumbar vertebral osteomyelitis: A case report.Medicine (Baltimore). 2018 May;97(18):e0682. doi: 10.1097/MD.0000000000010682. Medicine (Baltimore). 2018. PMID: 29718896 Free PMC article.
-
A case of back pain caused by Salmonella spondylitis -A case report-.Korean J Anesthesiol. 2010 Dec;59 Suppl(Suppl):S233-7. doi: 10.4097/kjae.2010.59.S.S233. Epub 2010 Dec 31. Korean J Anesthesiol. 2010. PMID: 21286449 Free PMC article.
References
-
- Maiuri F, Iaconetta G, Gallicchio B, Manto A, Briganti F. Spondylodiskitis. Clinical and magnetic resonance diagnosis. Spine. 1997;22:1741–1746. - PubMed
-
- Govender S, Parbhoo AH, Rasool MN, Maharaj J. Salmonella typhi spondylitis. J Pediatr Orthop. 1999;19:710–714. - PubMed
-
- Acharya S, Bhatnagar P. Salmonella spinal osteomyelitis: a case report and review of literature. Neurol India. 2004;52:499–500. - PubMed
-
- Wu KC, Yao TC, Yeh KW, Huang JL. Osteomyelitis in patients with systemic lupus erythematosus. J Rheumatol. 2004;31:1340–1343. - PubMed
-
- Santos EM, Sapico FL. Vertebral osteomyelitis due to Salmonella: report of two cases and review. Clin Infect Dis. 1998;27:287–295. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials