

Respiratory failure in acute organophosphorus pesticide self-poisoning
- PMID: 16861715
- PMCID: PMC1525210
- DOI: 10.1093/qjmed/hcl065
Respiratory failure in acute organophosphorus pesticide self-poisoning
Abstract
Background: Acute organophosphorus (OP) pesticide poisoning is a major clinical problem in the developing world. Textbooks ascribe most deaths to respiratory failure occurring in one of two distinct clinical syndromes: acute cholinergic respiratory failure or the intermediate syndrome. Delayed failure appears to be due to respiratory muscle weakness, but its pathophysiology is unclear.
Aim: To describe the clinical patterns of OP-induced respiratory failure, and to determine whether the two syndromes are clinically distinct.
Design: Prospective study of 376 patients with confirmed OP poisoning.
Methods: Patients were observed throughout their admission to three Sri Lankan hospitals. Exposure was confirmed by butyrylcholinesterase and blood OP assays.
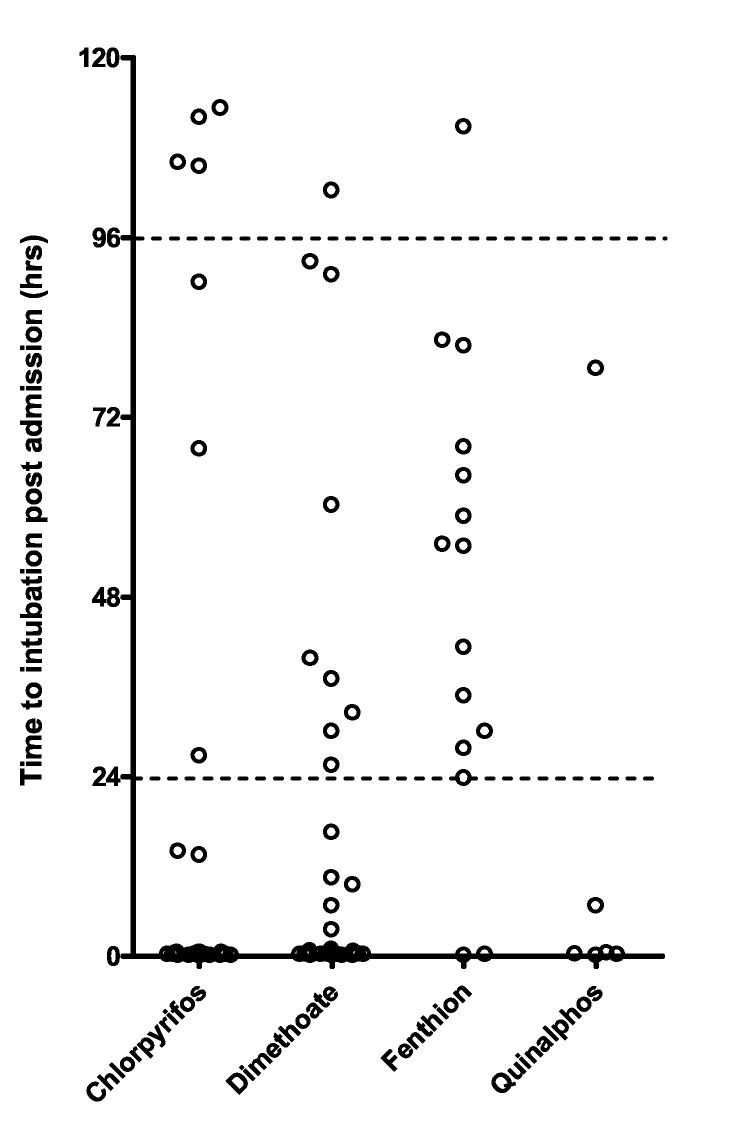
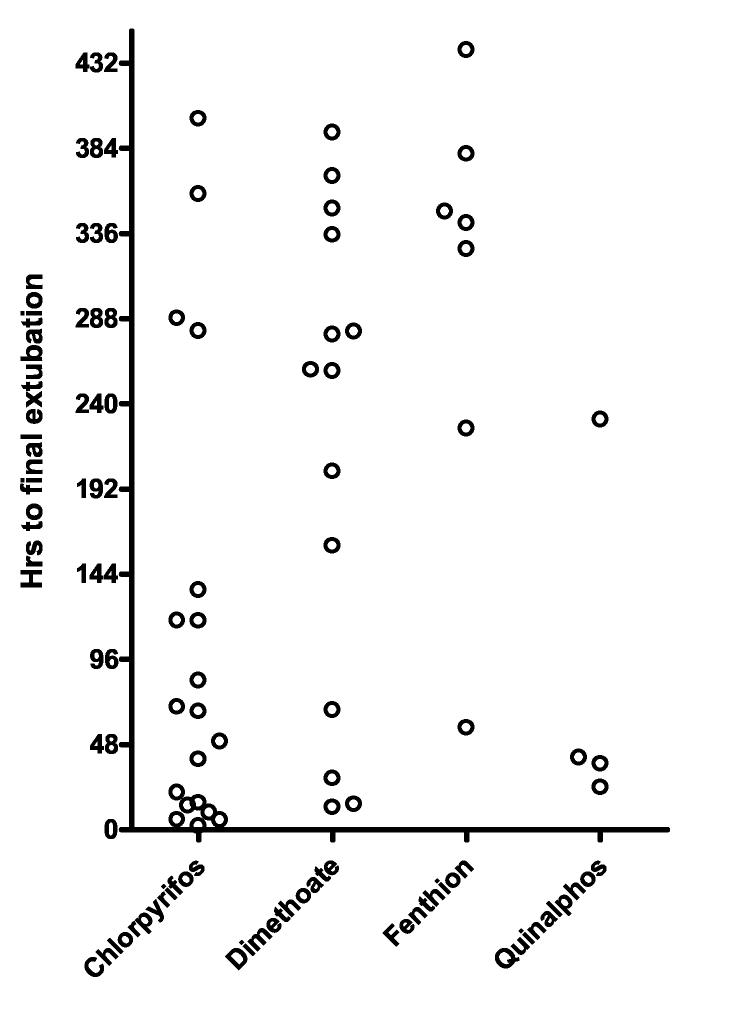
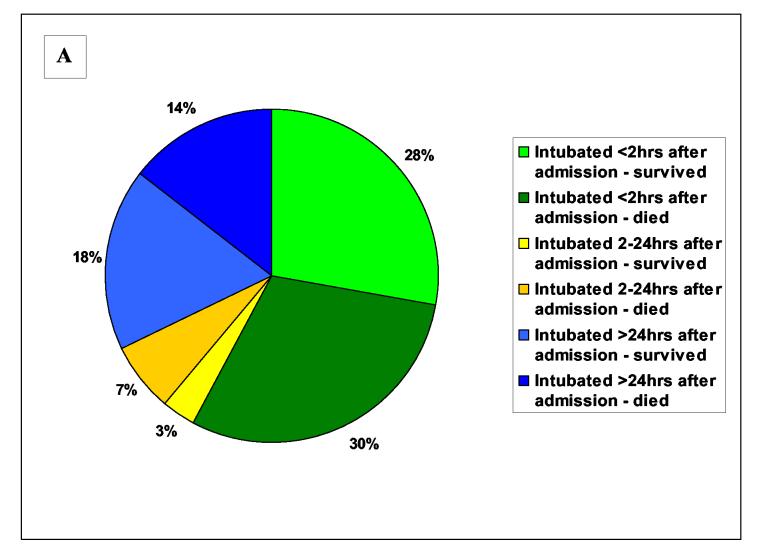
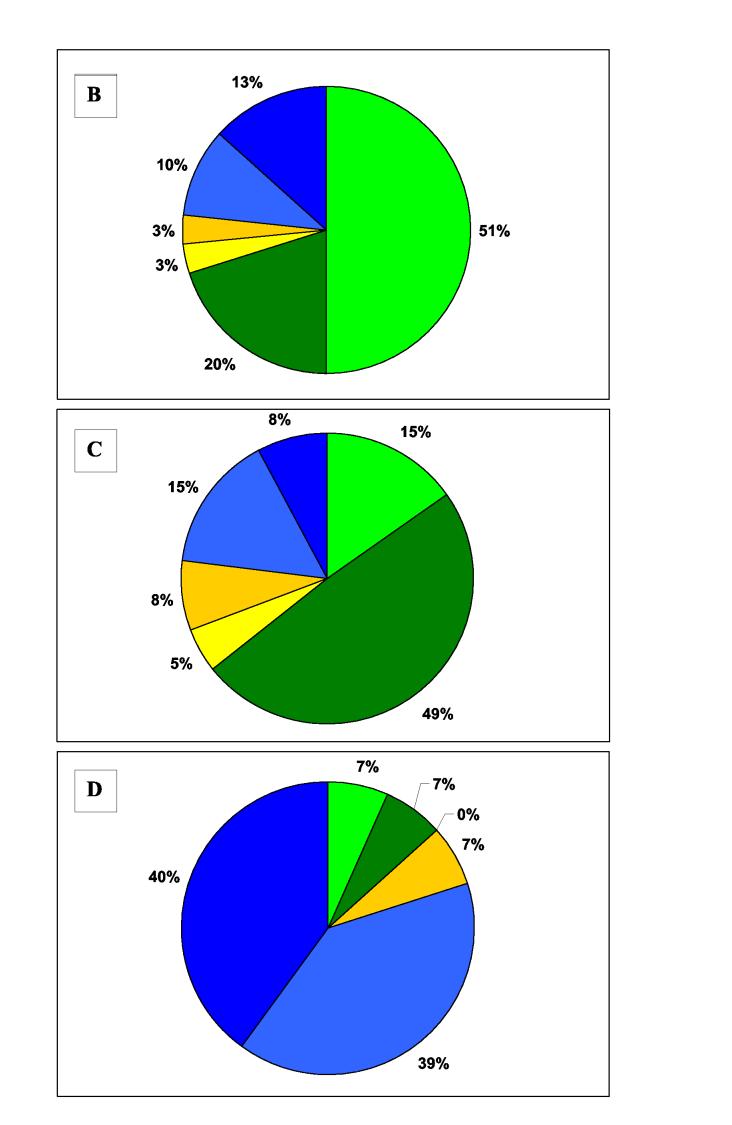
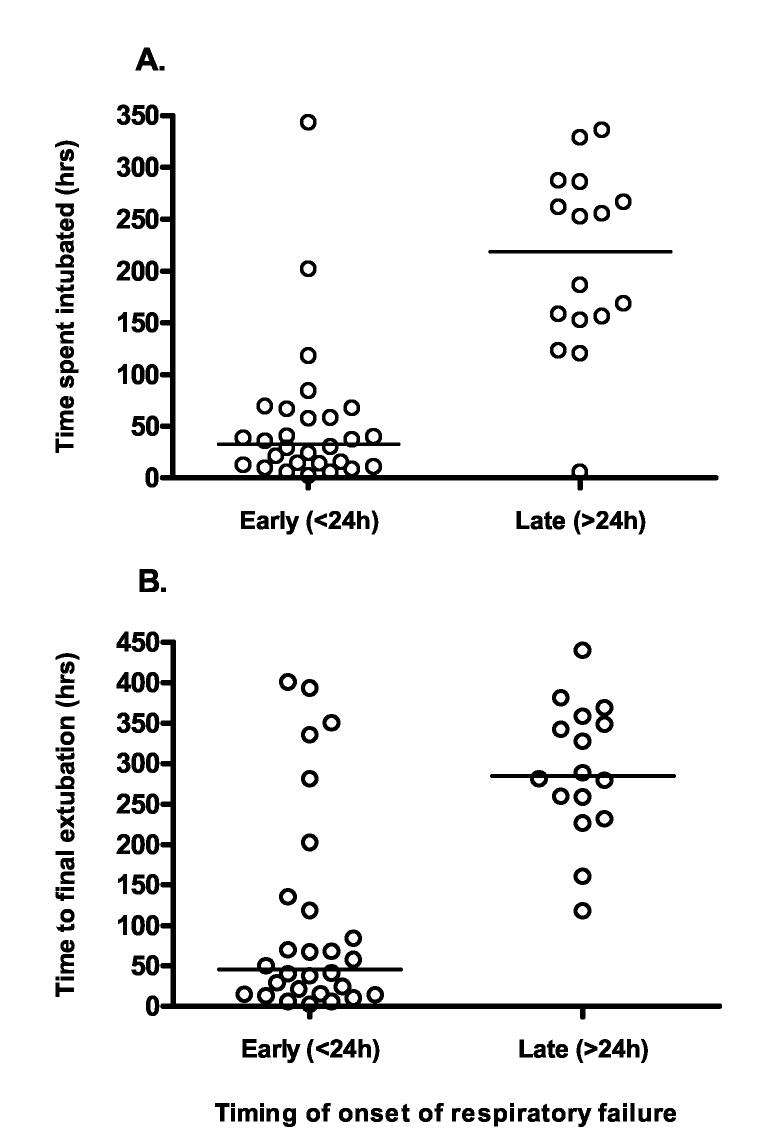
Results: Ninety of 376 patients (24%) required intubation: 52 (58%) within 2 h of admission while unconscious with cholinergic features. Twenty-nine (32%) were well on admission but then required intubation after 24 h while conscious and without cholinergic features. These two syndromes were not clinically distinct and had much overlap. In particular, some patients who required intubation on arrival subsequently recovered consciousness but could not be extubated, requiring ventilation for up to 6 days.
Discussion: Respiratory failure did not occur as two discrete clinical syndromes within distinct time frames. Instead, the pattern of failure was variable and overlapped in some patients. There seemed to be two underlying mechanisms (an early acute mixed central and peripheral respiratory failure, and a late peripheral respiratory failure) rather than two distinct clinical syndromes.
Figures
References
-
- World Health Organization . Public health impact of pesticides used in agriculture. 0 edn WHO; Geneva: 1990.
-
- van der Hoek W, Konradsen F, Athukorala K, Wanigadewa T. Pesticide poisoning: a major health problem in Sri Lanka. Soc Sci Med. 1998;46:495–504. - PubMed
-
- Langley R, Sumner D. Pesticide mortality in the United States, 1979-1998. Vet Hum Toxicol. 2002;44:101–5. - PubMed
-
- Thiermann H, Szinicz L, Eyer F, Worek F, Eyer P, Felgenhauer N, Zilker T. Modern strategies in therapy of organophosphate poisoning. Toxicol Lett. 1999;107:233–9. - PubMed
-
- Bruyndonckx RB, Meulemans AI, Sabbe MB, Kumar AA, Delooz HH. Fatal intentional poisoning cases admitted to the University Hospitals of Leuven, Belgium, from 1993 to 1996. Eur J Emerg Med. 2002;9:238–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
