

Prospects for advancing tuberculosis control efforts through novel therapies
- PMID: 16866578
- PMCID: PMC1523376
- DOI: 10.1371/journal.pmed.0030273
Prospects for advancing tuberculosis control efforts through novel therapies
Abstract
Background: Development of new, effective, and affordable tuberculosis (TB) therapies has been identified as a critical priority for global TB control. As new candidates emerge from the global TB drug pipeline, the potential impacts of novel, shorter regimens on TB incidence and mortality have not yet been examined.
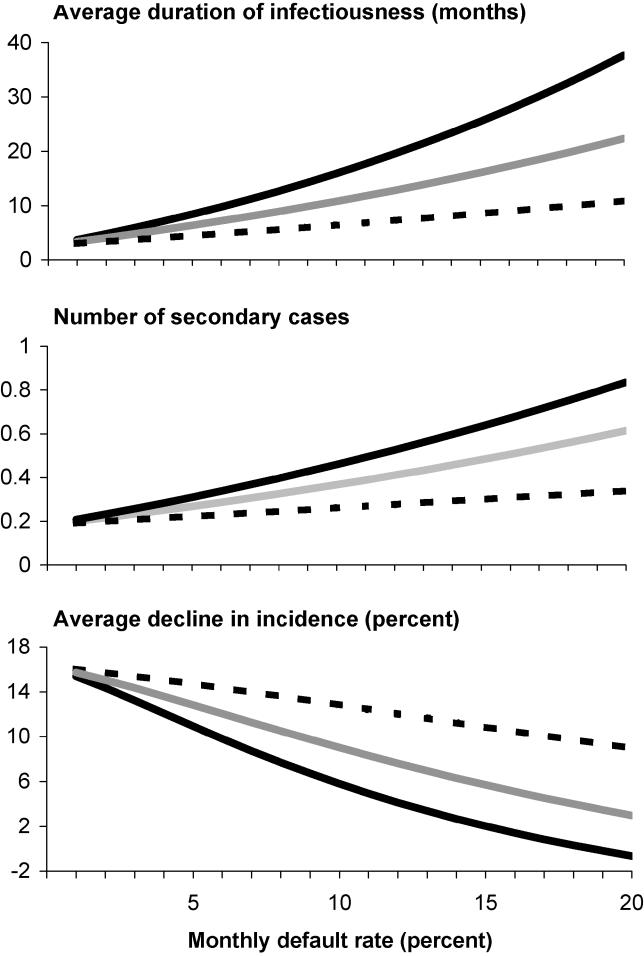
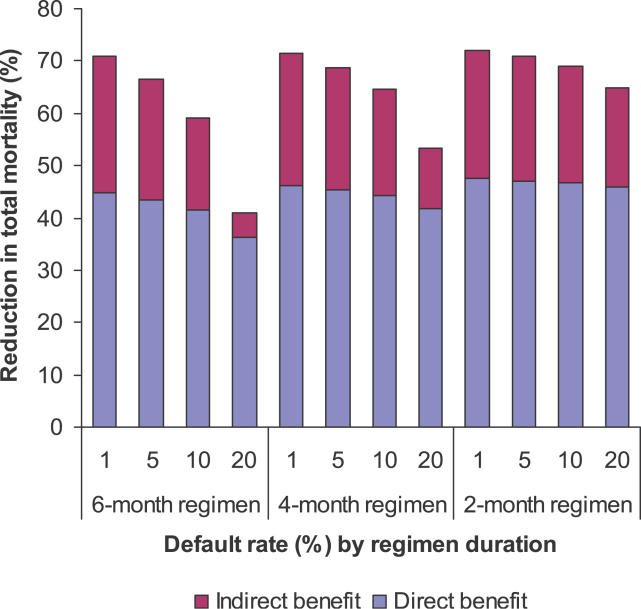
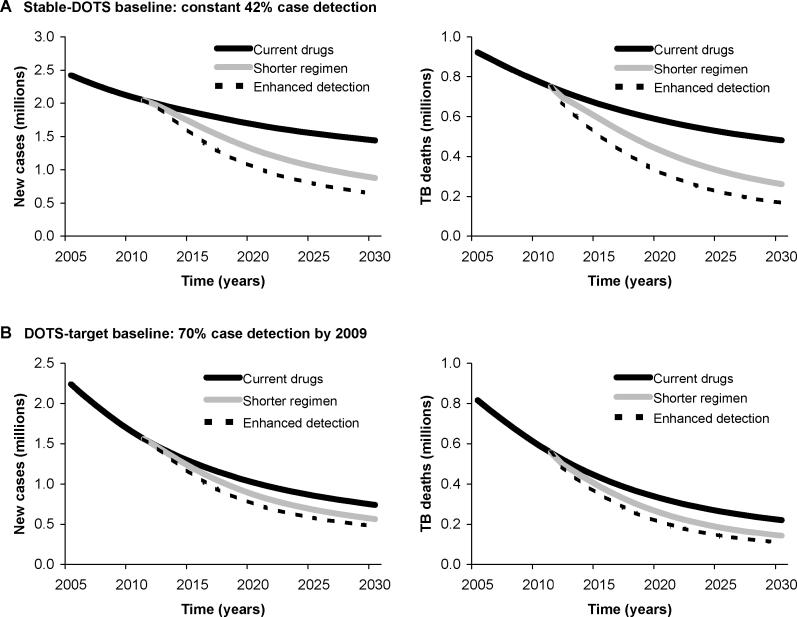
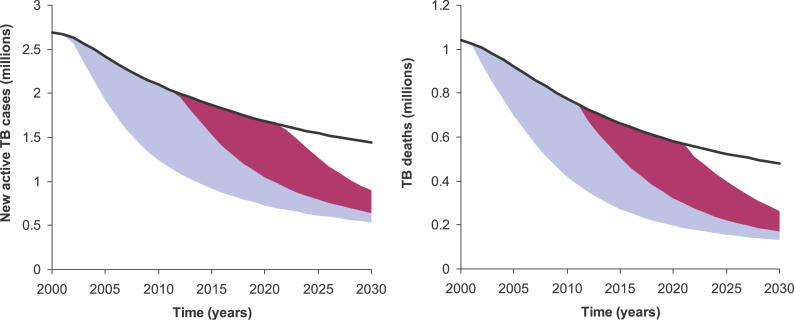
Methods and findings: We used a mathematical model of TB to evaluate the expected benefits of shortening the duration of effective chemotherapy for active pulmonary TB. First, we considered general relationships between treatment duration and TB dynamics. Next, as a specific example, we calibrated the model to reflect the current situation in the South-East Asia region. We found that even with continued and rapid progress in scaling up the World Health Organization's DOTS strategy of directly observed, short-course chemotherapy, the benefits of reducing treatment duration would be substantial. Compared to a baseline of continuing DOTS coverage at current levels, and with currently available tools, a 2-mo regimen introduced by 2012 could prevent around 20% (range 13%-28%) of new cases and 25% (range 19%-29%) of TB deaths in South-East Asia between 2012 and 2030. If effective treatment with existing drugs expands rapidly, overall incremental benefits of shorter regimens would be lower, but would remain considerable (13% [range 8%-19%] and 19% [range 15%-23%] reductions in incidence and mortality, respectively, between 2012 and 2030). A ten-year delay in the introduction of new drugs would erase nearly three-fourths of the total expected benefits in this region through 2030.
Conclusions: The introduction of new, shorter treatment regimens could dramatically accelerate the reductions in TB incidence and mortality that are expected under current regimens-with up to 2- or 3-fold increases in rates of decline if shorter regimens are accompanied by enhanced case detection. Continued progress in reducing the global TB burden will require a balanced approach to pursuing new technologies while promoting wider implementation of proven strategies.
Conflict of interest statement
Figures
Comment in
-
Novel therapies for tuberculosis: tuberculosis control and its discontents.PLoS Med. 2006 Oct;3(10):e461. doi: 10.1371/journal.pmed.0030461. PLoS Med. 2006. PMID: 17076574 Free PMC article. No abstract available.
References
-
- World Health Organization. WHO report 2005: Global tuberculosis control: Surveillance, planning and financing. Report number WHO/HTM/TB/2005.349. 2005.
-
- Styblo K, Meijer J, Sutherland I. Tuberculosis Surveillance Research Unit Report No. 1: The transmission of tubercle bacilli; its trend in a human population. Bull Int Union Tuberc. 1969;42:1–104. - PubMed
-
- Wilson LG. The historical decline of tuberculosis in Europe and America: Its causes and significance. J Hist Med Allied Sci. 1990;45:366–396. - PubMed
-
- Vynnycky E, Fine PE. The annual risk of infection with Mycobacterium tuberculosis in England and Wales since 1901. Int J Tuberc Lung Dis. 1997;1:389–396. - PubMed
-
- Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, et al. The growing burden of tuberculosis: Global trends and interactions with the HIV epidemic. Arch Intern Med. 2003;163:1009–1021. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
