

Respiratory dysfunction and management in spinal cord injury
- PMID: 16867197
- PMCID: PMC2495152
Respiratory dysfunction and management in spinal cord injury
Abstract
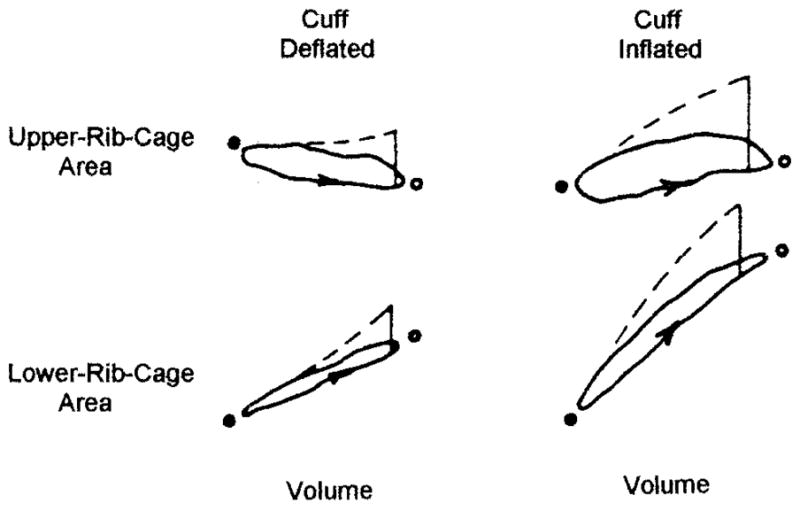
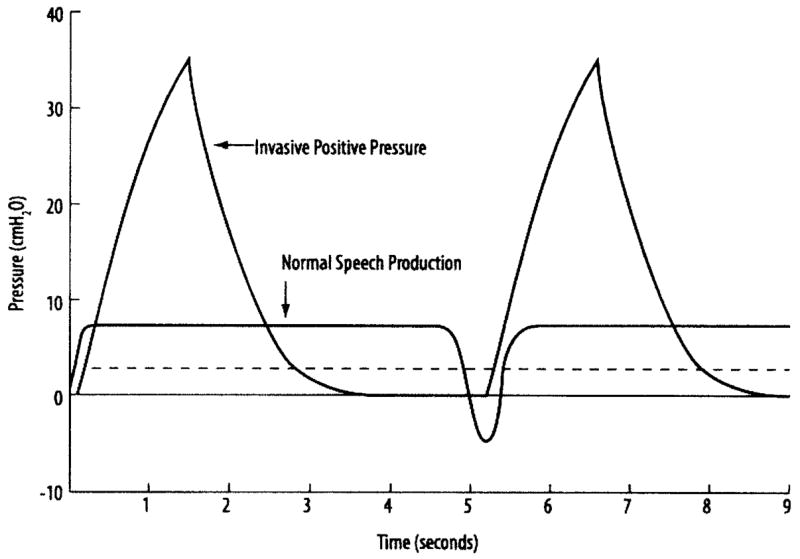
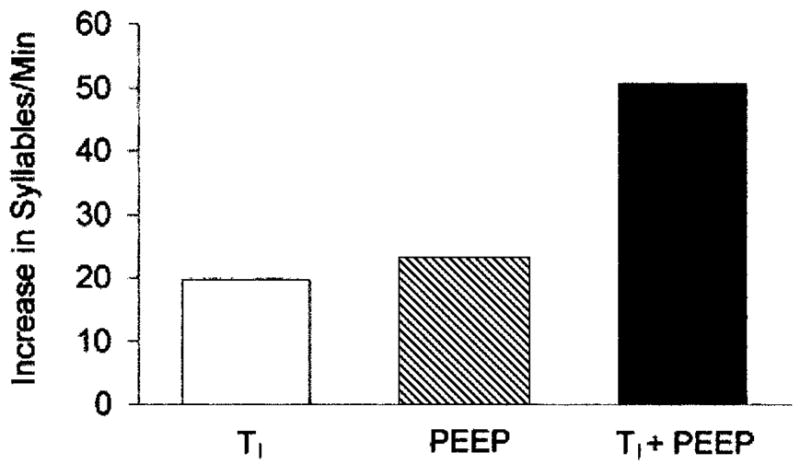
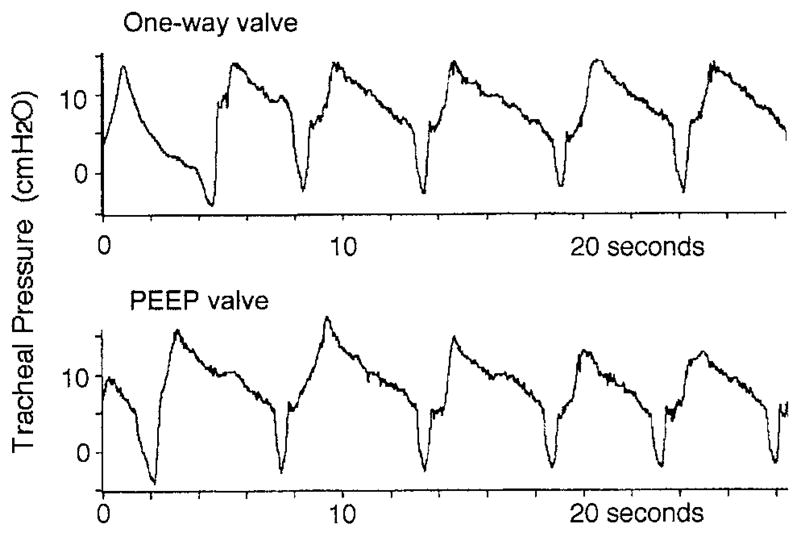
Respiratory dysfunction is a major cause of morbidity and mortality in spinal cord injury (SCI), which causes impairment of respiratory muscles, reduced vital capacity, ineffective cough, reduction in lung and chest wall compliance, and excess oxygen cost of breathing due to distortion of the respiratory system. Severely affected individuals may require assisted ventilation, which can cause problems with speech production. Appropriate candidates can sometimes be liberated from mechanical ventilation by phrenic-nerve pacing and pacing of the external intercostal muscles. Partial recovery of respiratory-muscle performance occurs spontaneously. The eventual vital capacity depends on the extent of spontaneous recovery, years since injury, smoking, a history of chest injury or surgery, and maximum inspiratory pressure. Also, respiratory-muscle training and abdominal binders improve performance of the respiratory muscles. For patients on long-term ventilation, speech production is difficult. Often, practitioners are reluctant to deflate the tracheostomy tube cuff to allow speech production. Yet cuff-deflation can be done safely. Standard ventilator settings produce poor speech quality. Recent studies demonstrated vast improvement with long inspiratory time and positive end-expiratory pressure. Abdominal binders improve speech quality in patients with phrenic-nerve pacers. Recent data show that the level and completeness of injury and older age at the time of injury may not be related directly to mortality in SCI, which suggests that the care of SCI has improved. The data indicate that independent predictors of all-cause mortality include diabetes mellitus, heart disease, cigarette smoking, and percent-of-predicted forced expiratory volume in the first second. An important clinical problem in SCI is weak cough, which causes retention of secretions during infections. Methods for secretion clearance include chest physical therapy, spontaneous cough, suctioning, cough assistance by forced compression of the abdomen ("quad cough"), and mechanical insufflation-exsufflation. Recently described but not yet available for general use is activation of the abdominal muscles via an epidural electrode placed at spinal cord level T9-L1.
Figures
References
-
- Spinal cord injury: facts and figures at a glance. National Spinal Cord Injury Center Statistical Center, Birmingham, Alabama. J Spinal Cord Med. 2006;29(4):379–80. - PubMed
-
- ASIA impairment scale, clinical syndromes, and standard neurological classification of spinal cord injury. http://www.asia-spinalinjury.org/publications/index.html.
-
- Scanlon PD, Loring SH, Pichurko BM, McCool FD, Slutsky AS, Sarkarati M, Brown R. Respiratory mechanics in acute quadriplegia: lung and chest wall compliance and dimensional changes during respiratory maneuvers. Am Rev Respir Dis. 1989;139(3):615–620. - PubMed
-
- Sharp JT, Sweany SK, VanLith P. Physiologic observations in diffuse pulmonary fibrosis and granulomatosis. Am Rev Respir Dis. 1966;94(3):316–331. - PubMed
-
- Gibson GJ, Pride NB. Lung distensibility: the static pressure-volume curve of the lungs and its use in clinical assessment. Br J Dis Chest. 1976;70(3):143–184. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical