

Clinical improvement and radiological progression in a girl with early onset scoliosis (EOS) treated conservatively--a case report
- PMID: 16872503
- PMCID: PMC1559640
- DOI: 10.1186/1748-7161-1-13
Clinical improvement and radiological progression in a girl with early onset scoliosis (EOS) treated conservatively--a case report
Abstract
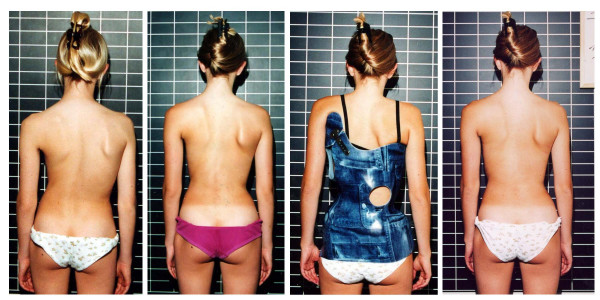
Background: Chêneau-Brace treatment of a certain standard reduces the rate of surgery, prevents progression and in a certain patient population leads to marked improvement of Cobb angle and cosmetic appearance. During the last two years a patient refusing surgery with a double major curvature of initially 60 degrees showed a clear cosmetic improvement and a clear radiological progression at the same time. The findings of this patient have been reviewed in order to find out how cosmetic appearance and Cobb angle can develop differently.
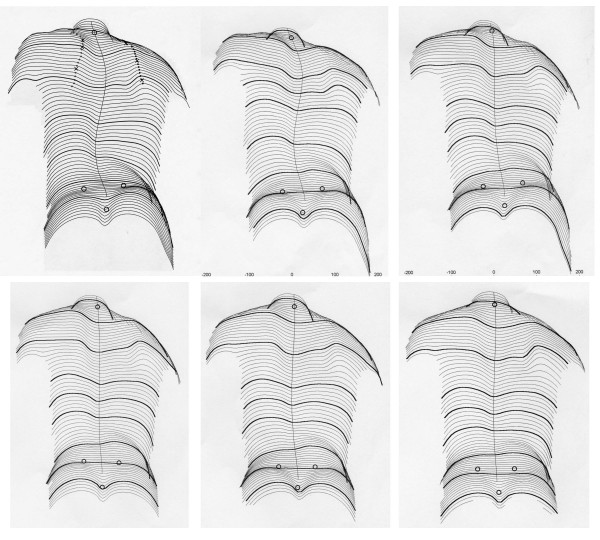
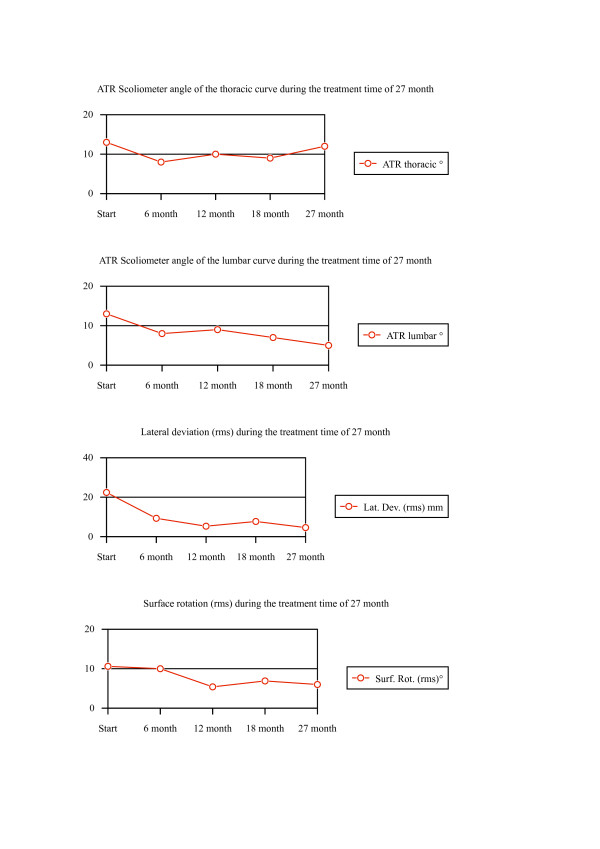
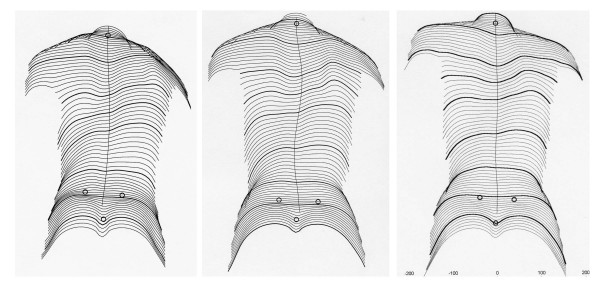
Methods: The patient entered conservative treatment at the age of 13 years, premenarchial with Tanner II and a Cobb angle of 60 degrees thoracic and 59 degrees lumbar. The angle of trunk rotation (ATR; Scoliometer) was 13 degrees thoracic and 13 degrees lumbar. We have documented the findings of this patient (Surface topography, ATR, Cobb angles and angles of vertebral rotation (according to Raimondi) during the treatment period (27 Month) until 2 years after the onset of menarche.
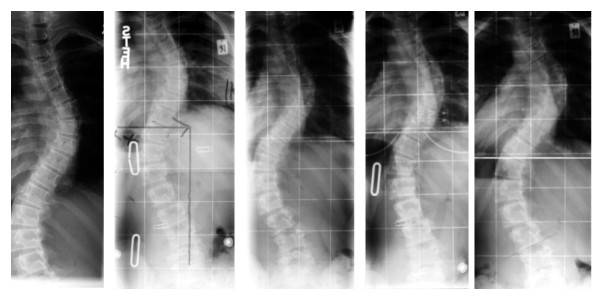
Results: After a treatment time of 27 Month the Cobb angle increased to 74 degrees thoracic and 65 degrees lumbar. The angles of vertebral rotation according to Raimondi increased slightly from 26 degrees thoracic and 28 degrees lumbar to 30 degrees thoracic and 28 degrees lumbar. The ATR improved to 12 degrees thoracic and 5 degrees lumbar while Lateral deviation improved from 22.4 mm to 4.6 mm and average surface rotation improved from 10.6 degrees to 6 degrees. In the X-rays a reduction of decompensation was visible. The patient felt comfortable with the cosmetic result.
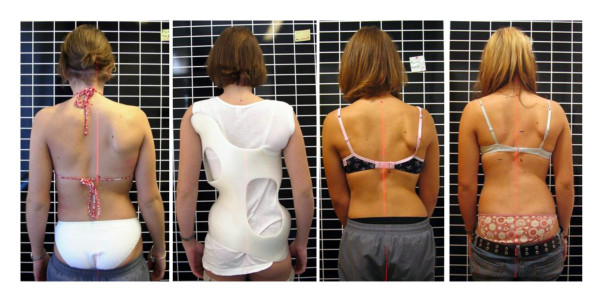
Conclusion: Conservative treatment may improve cosmetic appearance while the curve progresses radiologically. This could be explained by assuming that (1) the Rigo Chêneau brace is able to improve cosmetic appearance by changing the shape of the thorax when the curve itself is too stiff to be corrected by a brace, that (2) reduction of decompensation leads to significant cosmetical improvements or (3) that the patient gained weight and therefore the deformation is masked. However, the weight the patient gained cannot explain the cosmetical improvement in this case. Conservative treatment with a certain standard of quality seems a viable alternative for patients with Cobb angles of > 60 degrees when surgical treatment is refused. Specialists in scoliosis management should be aware of the fact that curve progression can occur even if the clinical measurements show an improvement.
Figures
Similar articles
-
Discrepancy in clinical versus radiological parameters describing deformity due to brace treatment for moderate idiopathic scoliosis.Scoliosis. 2007 Dec 3;2:18. doi: 10.1186/1748-7161-2-18. Scoliosis. 2007. PMID: 18053172 Free PMC article.
-
The effectiveness of selective thoracic fusion for treating adolescent idiopathic scoliosis: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Nov;13(11):4-16. doi: 10.11124/jbisrir-2015-2338. JBI Database System Rev Implement Rep. 2015. PMID: 26657460
-
Effect of the Chêneau Brace in the Natural History of Moderate Adolescent Idiopathic Scoliosis in Girls: Cohort Analysis of a Selected Homogenous Population of 100 Consecutive Skeletally Immature Patients.Spine Deform. 2018 Sep-Oct;6(5):514-522. doi: 10.1016/j.jspd.2018.01.006. Spine Deform. 2018. PMID: 30122386
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Management of spinal deformity in cerebral palsy: conservative treatment.J Child Orthop. 2013 Nov;7(5):415-8. doi: 10.1007/s11832-013-0516-5. Epub 2013 Aug 30. J Child Orthop. 2013. PMID: 24432104 Free PMC article. Review.
Cited by
-
Monitoring curve progression in adolescent idiopathic scoliosis, assessment of the diagnostic performance of rasterstereography in brace-treated and untreated patients.Eur Spine J. 2025 Aug 14. doi: 10.1007/s00586-025-09213-0. Online ahead of print. Eur Spine J. 2025. PMID: 40804498
-
Discrepancy in clinical versus radiological parameters describing deformity due to brace treatment for moderate idiopathic scoliosis.Scoliosis. 2007 Dec 3;2:18. doi: 10.1186/1748-7161-2-18. Scoliosis. 2007. PMID: 18053172 Free PMC article.
-
First end-result of a prospective cohort with AIS treated with a CAD Chêneau style brace.J Phys Ther Sci. 2019 Dec;31(12):983-991. doi: 10.1589/jpts.31.983. Epub 2019 Dec 3. J Phys Ther Sci. 2019. PMID: 32038069 Free PMC article.
-
Brace related stress in scoliosis patients - Comparison of different concepts of bracing.Scoliosis. 2007 Aug 20;2:10. doi: 10.1186/1748-7161-2-10. Scoliosis. 2007. PMID: 17708766 Free PMC article.
-
Corrective bracing for severe idiopathic scoliosis in adolescence: influence of brace on trunk morphology.ScientificWorldJournal. 2012;2012:435158. doi: 10.1100/2012/435158. Epub 2012 Apr 30. ScientificWorldJournal. 2012. PMID: 22666119 Free PMC article.
References
-
- Klisic P, Nikolic Z. Attitudes scoliotiques et scolioses idiopathiques: prévention à l'école. Personal communication. Journées Internationales sur la prévention des scolioses à l'âge scolaire Rome. 1982.
-
- Mollon G, Rodot JC. Scolioses structurales mineures et kinesithérapie. Etude statistique comparative et résultats. Kinésithér Scient. 1986;244:47–56.
-
- Rigo M, Quera-Salvá G, Puigdevall N. Effect of the exclusive employment of physiotherapy in patients with idiopathic scoliosis. Retrospective study. Proceedings of the 11th International Congress of the World Confederation For Physical Therapy London. pp. 1319–1321. 28 July – 2 August 1991.
-
- Weiss HR, Rigo M. Befundgerechte Physiotherapie bei Skoliose. Pflaum, Munich; 2001.
-
- Pauschert R, Niethard F. Ergebnisse der krankengymnastischen Behandlung auf neurophysiologischer Grundlage bei idiopathischer Skoliose: Eine prospektive Analyse. In: Weiss HR, editor. Wirbelsäulendeformitäten Band 3. Springer, Stuttgart; 1994. pp. 47–51.
LinkOut - more resources
Full Text Sources
Miscellaneous
