

Correlation of cavitation with ultrasound enhancement of thrombolysis
- PMID: 16875959
- PMCID: PMC1937506
- DOI: 10.1016/j.ultrasmedbio.2006.04.008
Correlation of cavitation with ultrasound enhancement of thrombolysis
Abstract
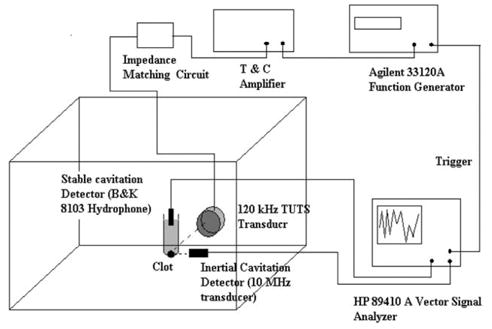
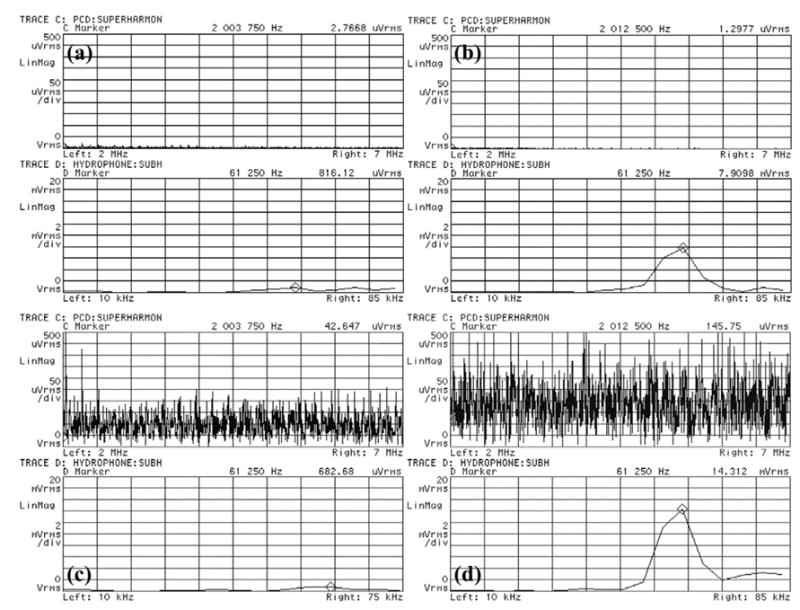
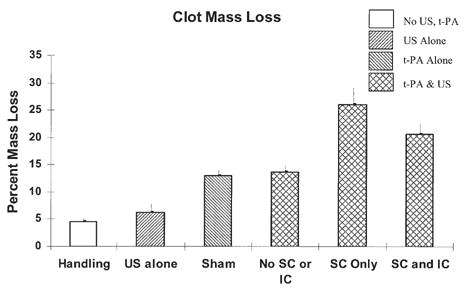
Pulsed ultrasound, when used as an adjuvant to recombinant tissue plasminogen activator (rt-PA), has been shown to enhance thrombolysis in the laboratory as well as in clinical trials for the treatment of ischemic stroke. The exact mechanism of this enhancement has not yet been elucidated. In this work, stable and inertial cavitation (SC and IC) are investigated as possible mechanisms for this enhancement. A passive cavitation detection scheme was utilized to measure cavitation thresholds at 120 kHz (80% duty cycle, 1667 Hz pulse repetition frequency) for four host fluid and sample combinations: plasma, plasma with rt-PA, plasma with clot and plasma with clot and rt-PA. Following cavitation threshold determination, clots were exposed to pulsed ultrasound for 30 min in vitro using three separate ultrasound treatment regimes: (1) no cavitation (0.15 MPa), (2) SC alone (0.24 MPa) or (3) SC + IC combined (0.36 MPa) in the presence of rt-PA. Percent clot mass loss after each treatment was used to determine thrombolysis efficacy. The highest percent mass loss was observed in the stable cavitation regime (26%), followed by the combined stable and inertial cavitation regime (20.7%). Interestingly, the percent mass loss in clots exposed to ultrasound without cavitation (13.7%) was not statistically significantly different from rt-PA alone (13%) [p > 0.05]. Significant enhancement of thrombolysis correlates with presence of cavitation and stable cavitation appears to play a more important role in the enhancement of thrombolysis. (E-mail: ).
Figures

References
-
- Akiyama M, Ishibashi T, Yamada T, Furuhata H. Low frequency ultrasound penetrates the cranium and enhances thrombolysis in vitro. Neurosurgery. 1998;43:828–833. - PubMed
-
- Alexandrov AV, Molina CA, Grotta JC, et al. Ultrasound-enhanced systemic thrombolysis for acute ischemic stroke. N Engl J Med. 2004;351(21):2170–2178. - PubMed
-
- Alexandrov AV, Demchul AM, Burgin WS, et al. Ultrasound-enhanced thrombolysis for acute ischemic stroke: Phase I. Findings of the CLOTBUST trial. J Neuroimaging. 2004;14(2):113–117. - PubMed
-
- ANSI Technical Report—Bubble detection and Cavitation Monitoring. ANSI. S1.24:TR-2002.
-
- Apfel RE. Acoustic cavitation prediction. J Acoust Soc Am. 1981;69:1624–1633.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
