

Symptomatic anomalous origination of the left coronary artery from the opposite sinus of valsalva. Clinical presentations, diagnosis, and surgical repair
- PMID: 16878619
- PMCID: PMC1524694
Symptomatic anomalous origination of the left coronary artery from the opposite sinus of valsalva. Clinical presentations, diagnosis, and surgical repair
Abstract
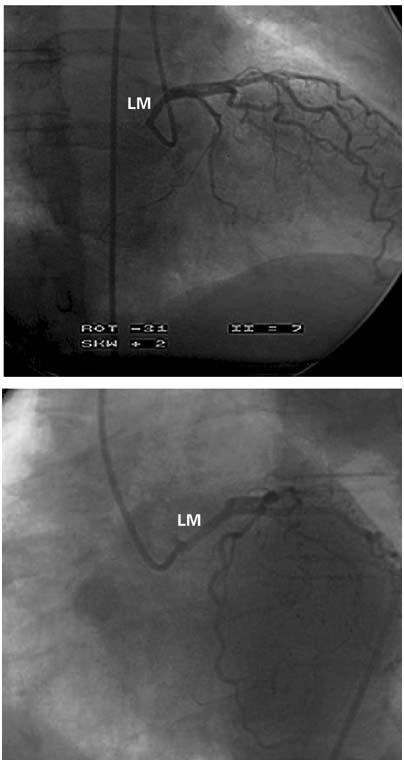
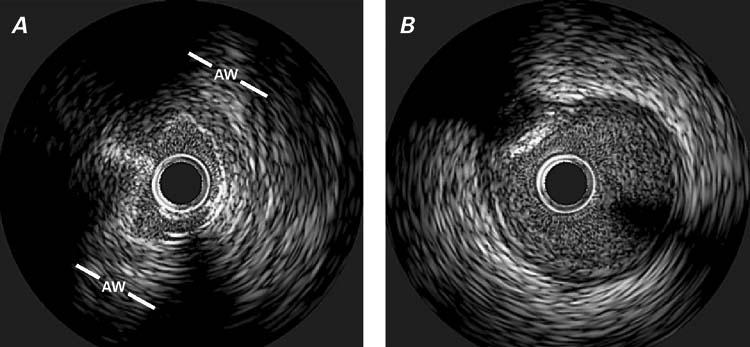
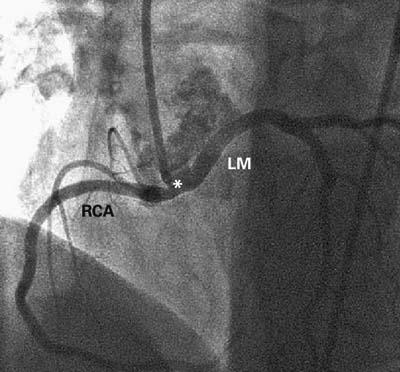
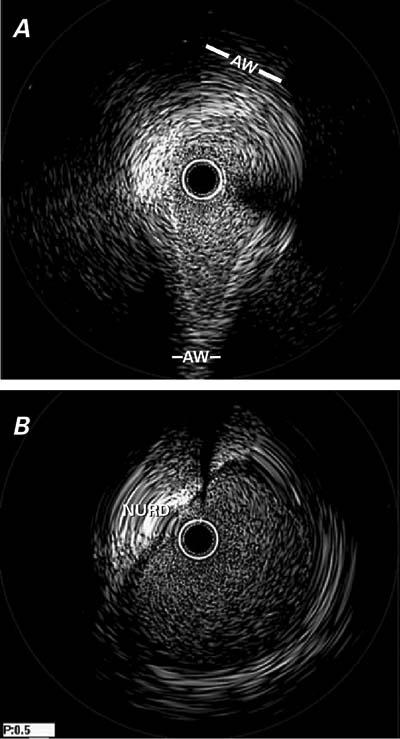
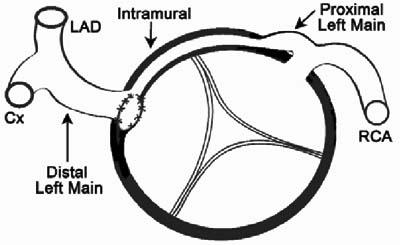
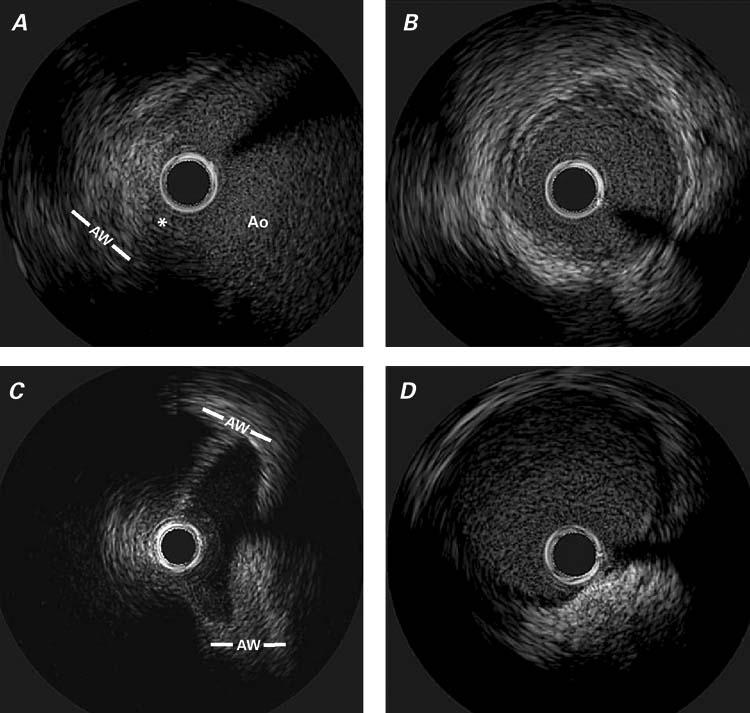
Anomalous origination of a coronary artery can have serious, even fatal, consequences. Intravascular ultrasonography has recently provided new insights into anomalous coronary artery origination from the opposite sinus of Valsalva. On the basis of these insights, we describe 3 typical forms of this anomaly with left coronary artery involvement, including clinical presentations, diagnostic methods (particularly intravascular ultrasonography), and details of surgical treatment. In this case series, the left coronary artery originated from the noncoronary sinus in 1 patient and from the right sinus in another patient. In the 3rd patient, both the left and right coronary arteries originated from the ascending aorta above the sinotubular junction. Baseline areas of stenosis ranged from 48.6% to 70.1%. Intravascular ultrasonography was the only method that enabled us to clarify the mechanisms and the severity of the anomaly. Pharmacologic challenge was useful to predict worsening that might have occurred under physiologic conditions. We found that, in cases of symptomatic left anomalous coronary artery origination from the opposite sinus of Valsalva, the proximal segment of the left coronary artery consistently has (1) an intramural course inside the aortic wall; (2) hypoplasia, as determined by its circumference; and (3) a cross-sectional ovaloid deformity (lateral compression) with phasic and exercise-induced worsening of the deformity With regard to surgical treatment, ostioplasty is preferable to coronary bypass. To establish sound guidelines for managing these anomalies, a larger series should be studied prospectively with quantitative parameters and long-term follow-up.
Figures

References
-
- Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation 2002;105:2449–54. - PubMed
-
- Cheitlin MD, De Castro CM, McAllister HA. Sudden death as a complication of anomalous left coronary origin from the anterior sinus of Valsalva. A not-so-minor congenital anomaly. Circulation 1974;50:780–7. - PubMed
-
- Taylor AJ, Byers JP, Cheitlin MD, Virmani R. Anomalous right or left coronary artery from the contralateral coronary sinus: “high-risk” abnormalities in the initial coronary artery course and heterogeneous clinical outcomes. Am Heart J 1997;133:428–35. - PubMed
-
- Eckart RE, Scoville SL, Campbell CL, Shry EA, Stajduhar KC, Potter RN, et al. Sudden death in young adults: a 25-year review of autopsies in military recruits. Ann Intern Med 2004;141:829–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources