

Inhibitory autoantibodies against ADAMTS-13 in patients with thrombotic thrombocytopenic purpura bind ADAMTS-13 protease and may accelerate its clearance in vivo
- PMID: 16879212
- PMCID: PMC2577225
- DOI: 10.1111/j.1538-7836.2006.02025.x
Inhibitory autoantibodies against ADAMTS-13 in patients with thrombotic thrombocytopenic purpura bind ADAMTS-13 protease and may accelerate its clearance in vivo
Abstract
Background: Many patients with acquired thrombotic thrombocytopenic purpura (TTP) harbor autoantibodies that may bind and/or inhibit ADAMTS-13 proteolytic activity and accelerate its clearance in vivo.
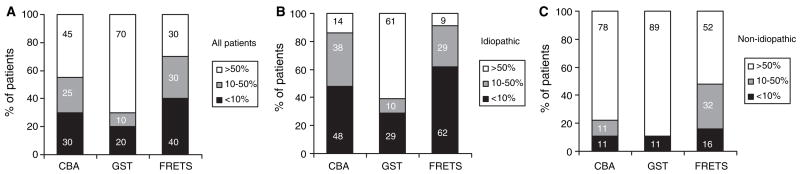
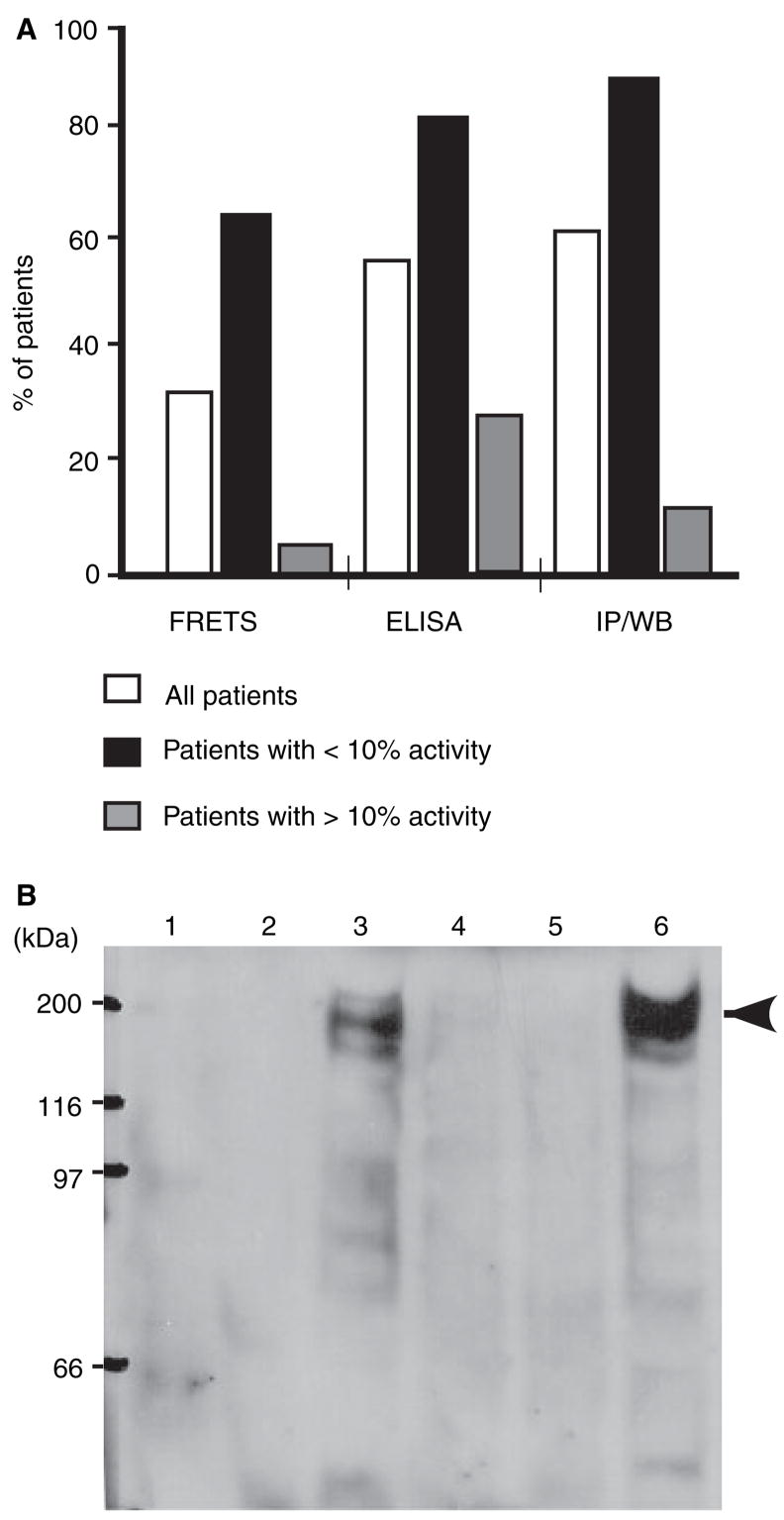
Methods: To test this hypothesis, we determined ADAMTS-13 activity and antigen levels in parallel plasma samples from patients clinically diagnosed with TTP. Collagen binding, GST-VWF73 and FRETS-VWF73 assays were used to determine ADAMTS-13 activity and to detect inhibitory autoantibodies. Enzyme-linked immunosorbent assay (ELISA) and immunoprecipitation plus Western blotting (IP/WB) were used to detect total anti-ADAMTS-13 IgG (inhibitory and non-inhibitory).
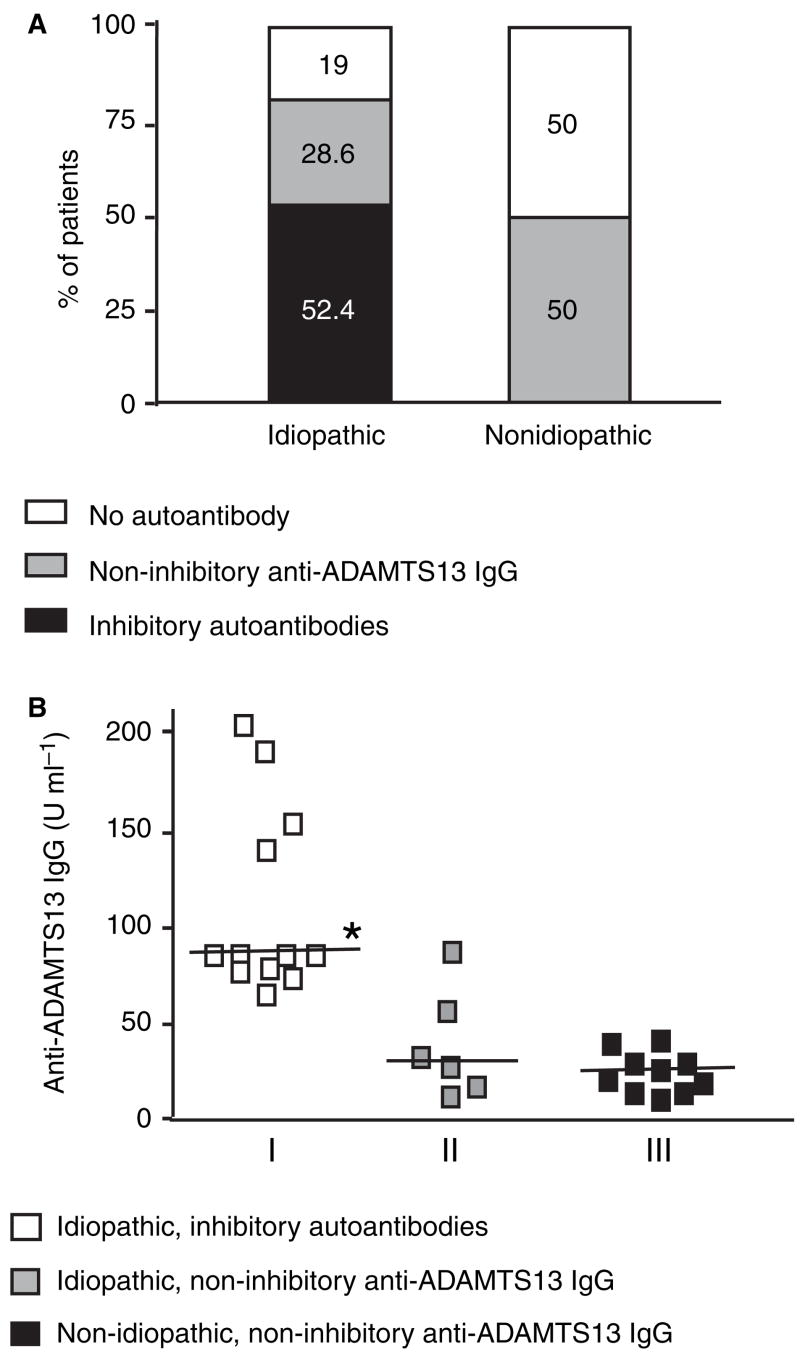
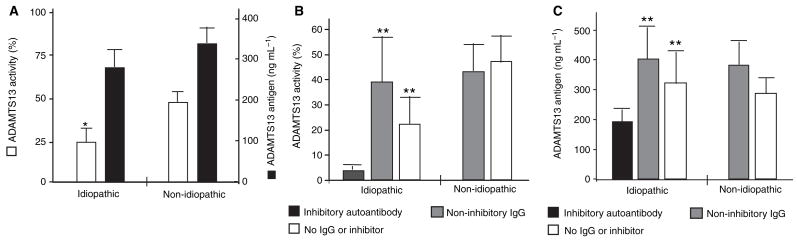
Results: Among 40 patients with TTP (21 idiopathic and 19 non-idiopathic), inhibitory autoantibodies were detected (by FRETS-VWF73) in 52% of idiopathic and 0% of non-idiopathic TTP patients. In contrast, non-inhibitory IgG autoantibodies were detected in 29% of idiopathic and 50% of non-idiopathic TTP patients. The concentration of inhibitory IgG autoantibody in idiopathic TTP patients was significantly higher than that of non-inhibitory IgG in either idiopathic or non-idiopathic TTP patients. Idiopathic TTP patients demonstrated significantly reduced ADAMTS-13 activity compared with non-idiopathic patients, but only slightly lower ADAMTS-13 antigen levels. Interestingly, patients with inhibitory autoantibodies exhibited significantly lower ADAMTS-13 antigen levels than those with only non-inhibitory IgG autoantibodies or no autoantibody. Serial plasma exchanges increased levels of ADAMTS-13 activity and antigen concurrently in patients with inhibitory autoantibodies.
Conclusion: The identification of severe ADAMTS-13 deficiency and autoantibodies or inhibitors appears to be assay-dependent; the inhibitory IgG autoantibodies, in addition to binding and inhibiting ADAMTS-13 proteolytic activity, may accelerate ADAMTS-13 clearance in vivo.
Figures


References
-
- Moake JL. Thrombotic thrombocytopenic purpura: the systemic clumping ‘plague’. Annu Rev Med. 2002;53:75–88. - PubMed
-
- Moake JL. Thrombotic microangiopathies. N Engl J Med. 2002;347:589–600. - PubMed
-
- Amorosi EL, Ultmann JE. Thrombocytopic purpura: report of 16 cases and review of the literature. Medicine (Baltimore) 1966;45:139– 59.
-
- Bell WR, Braine HG, Ness PM, Kickler TS. Improved survival in thrombotic thrombocytopenic purpura-hemolytic uremic syndrome. Clinical experience in 108 patients. N Engl J Med. 1991;325:398–403. - PubMed
-
- Rock GA, Shumak KH, Buskard NA, Blanchette VS, Kelton JG, Nair RC, Spaso RA. Comparison of plasma exchange with plasma infusion in the treatment of thrombotic thrombocytopenic purpura. Canadian Apheresis Study Group. N Engl J Med. 1991;325:393–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
