

Patient-centred screening for primary immunodeficiency: a multi-stage diagnostic protocol designed for non-immunologists
- PMID: 16879238
- PMCID: PMC1809674
- DOI: 10.1111/j.1365-2249.2006.03138.x
Patient-centred screening for primary immunodeficiency: a multi-stage diagnostic protocol designed for non-immunologists
Abstract
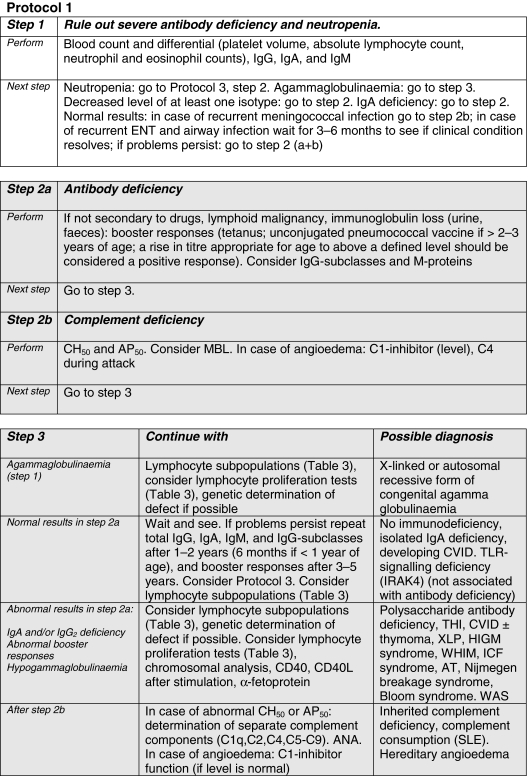
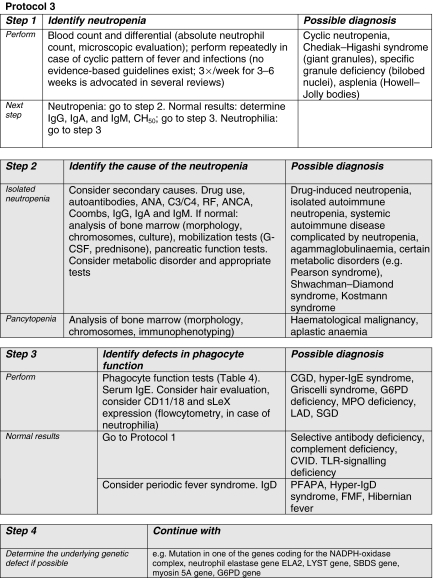
Efficient early identification of primary immunodeficiency disease (PID) is important for prognosis, but is not an easy task for non-immunologists. The Clinical Working Party of the European Society for Immunodeficiencies (ESID) has composed a multi-stage diagnostic protocol that is based on expert opinion, in order to increase the awareness of PID among doctors working in different fields. The protocol starts from the clinical presentation of the patient; immunological skills are not needed for its use. The multi-stage design allows cost-effective screening for PID within the large pool of potential cases in all hospitals in the early phases, while more expensive tests are reserved for definitive classification in collaboration with an immunologist at a later stage. Although many PIDs present in childhood, others may present at any age. The protocols presented here are therefore aimed at both adult physicians and paediatricians. While designed for use throughout Europe, there will be national differences which may make modification of this generic algorithm necessary.
Figures

Comment in
-
Early indicators of immunodeficiency in adults and children: protocols for screening for primary immunological defects.Clin Exp Immunol. 2006 Aug;145(2):201-3. doi: 10.1111/j.1365-2249.2006.03126.x. Clin Exp Immunol. 2006. PMID: 16879237 Free PMC article.
Similar articles
-
Patient-centred screening for primary immunodeficiency, a multi-stage diagnostic protocol designed for non-immunologists: 2011 update.Clin Exp Immunol. 2012 Jan;167(1):108-19. doi: 10.1111/j.1365-2249.2011.04461.x. Clin Exp Immunol. 2012. PMID: 22132890 Free PMC article. Review.
-
[Immunology in medical practice. XXXIV. Screening for suspected immunodeficiency: Introduction].Ned Tijdschr Geneeskd. 2000 Nov 11;144(46):2192-6. Ned Tijdschr Geneeskd. 2000. PMID: 11103255 Review. Dutch.
-
Early indicators of immunodeficiency in adults and children: protocols for screening for primary immunological defects.Clin Exp Immunol. 2006 Aug;145(2):201-3. doi: 10.1111/j.1365-2249.2006.03126.x. Clin Exp Immunol. 2006. PMID: 16879237 Free PMC article.
-
Evaluation of the Effectiveness of the 6 Warning Signs of the European Society for Immunodeficiencies for Primary Immunodeficiencies in Older Adults.Int Arch Allergy Immunol. 2024;185(4):402-410. doi: 10.1159/000535604. Epub 2024 Jan 12. Int Arch Allergy Immunol. 2024. PMID: 38219730
-
How effective are the 6 European Society of Immunodeficiency warning signs for primary immunodeficiency disease?Ann Allergy Asthma Immunol. 2016 Feb;116(2):151-155.e1. doi: 10.1016/j.anai.2015.12.001. Ann Allergy Asthma Immunol. 2016. PMID: 26815708
Cited by
-
Immune deficiency: changing spectrum of pathogens.Clin Exp Immunol. 2015 Aug;181(2):267-74. doi: 10.1111/cei.12600. Clin Exp Immunol. 2015. PMID: 25677249 Free PMC article.
-
Does this patient have an immunodeficiency?Clin Med (Lond). 2011 Aug;11(4):380-4. doi: 10.7861/clinmedicine.11-4-380. Clin Med (Lond). 2011. PMID: 21853840 Free PMC article. Review. No abstract available.
-
Recurrent or unusual infections in children - when to worry about inborn errors of immunity.Ther Adv Infect Dis. 2023 Apr 17;10:20499361231162978. doi: 10.1177/20499361231162978. eCollection 2023 Jan-Dec. Ther Adv Infect Dis. 2023. PMID: 37089444 Free PMC article. Review.
-
[Relevant cutaneous manifestations as indications for inborn errors of immunity].Dermatologie (Heidelb). 2024 Jul;75(7):577-586. doi: 10.1007/s00105-024-05331-w. Epub 2024 Jun 10. Dermatologie (Heidelb). 2024. PMID: 38856791 German.
-
Technical and diagnostic performance of five commercial anti-diphtheria toxoid IgG enzyme-linked immunosorbent assay kits.Clin Vaccine Immunol. 2010 Oct;17(10):1612-6. doi: 10.1128/CVI.00077-10. Epub 2010 Aug 25. Clin Vaccine Immunol. 2010. PMID: 20739499 Free PMC article.
References
-
- Notarangelo L, Casanova JL, Fischer A, et al. Primary immunodeficiency diseases: an update. J Allergy Clin Immunol. 2004;114:677–87. - PubMed
-
- Stiehm ER, Ochs HD, Winkelstein JA. Immunodeficiency disorders: general considerations. In: Stiehm ER, Ochs HD, Winkelstein JA, editors. Immunologic disorders in infants and children. 5. Philadelphia; 2004. pp. 289–355.
-
- Folds JD, Schmitz JL. Clinical and laboratory assessment of immunity. J Allergy Clin Immunol. 2003;111(2 Suppl):S702–11. - PubMed
-
- Bonilla FA, Bernstein IL, Khan DA, et al. American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology; Joint Council of Allergy, Asthma and Immunology. Practice parameter for the diagnosis and management of primary immunodeficiency. Ann Allergy Asthma Immunol. 2005;94(5 Suppl. 1):S1–63. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
