

Review
doi: 10.1186/cc4975.
Coagulation abnormalities in critically ill patients
Affiliations
- PMID: 16879728
- PMCID: PMC1750988
- DOI: 10.1186/cc4975
Item in Clipboard
Review
Coagulation abnormalities in critically ill patients
Crit Care.
2006.
Abstract
Many critically ill patients develop hemostatic abnormalities, ranging from isolated thrombocytopenia or prolonged global clotting tests to complex defects, such as disseminated intravascular coagulation. There are many causes for a deranged coagulation in critically ill patients and each of these underlying disorders may require specific therapeutic or supportive management. In recent years, new insights into the pathogenesis and clinical management of many coagulation defects in critically ill patients have been accumulated and this knowledge is helpful in determining the optimal diagnostic and therapeutic strategy.
Figures
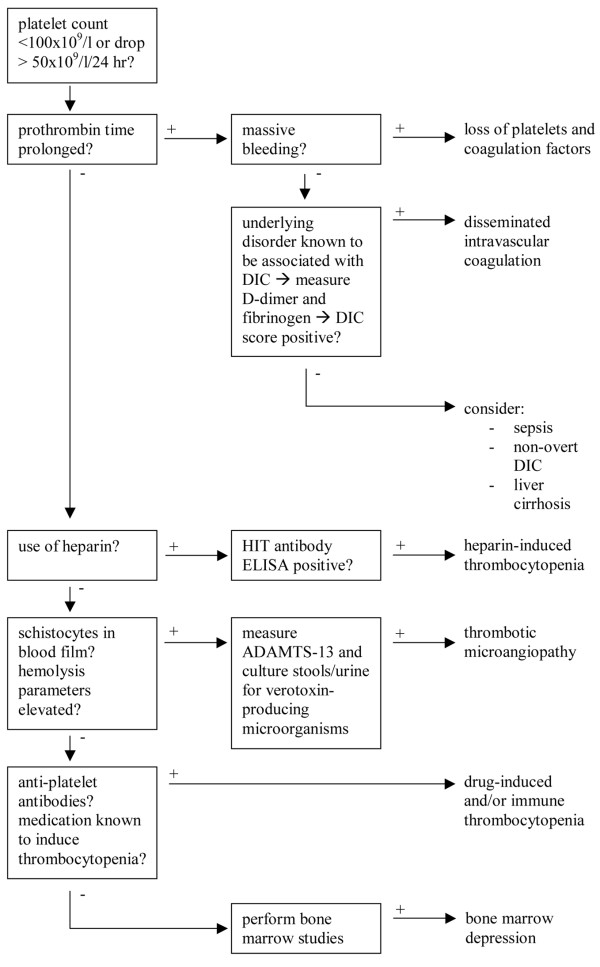
Differential diagnostic algorithm for coagulation abnormalities on the intensive care unit. DIC, disseminated intravascular coagulation; ELISA, enzyme-linked immunosorbent assay; HIT, heparin-induced thrombocytopenia.
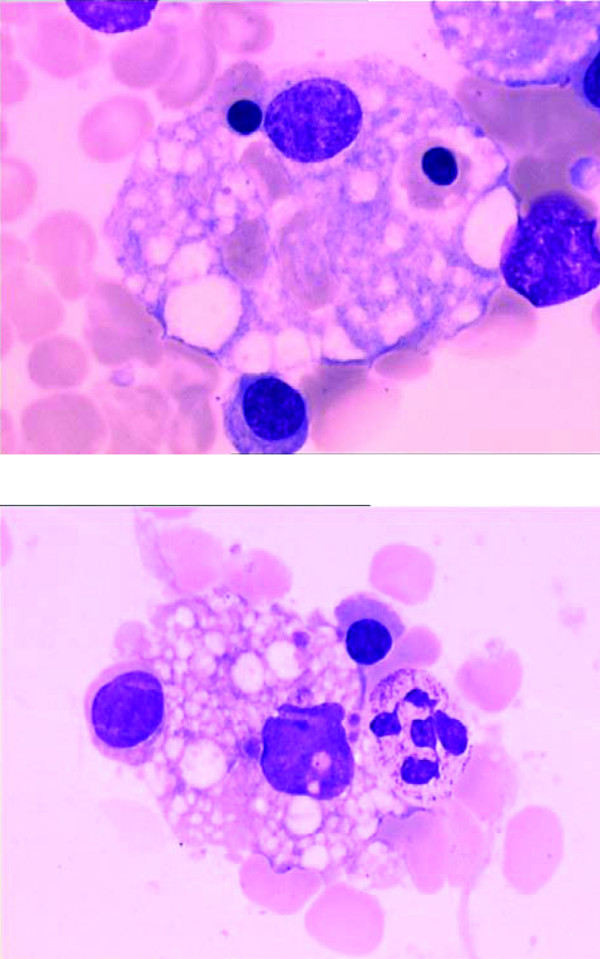
Typical examples of hematophagocytosis of bone marrow cells by macrophages. The bone marrow was obtained from a patient with severe sepsis (May-Grunwald-Giemsa staining, ×500). Courtesy of Bruno Francois and Frank Trimoreau, Dupuytren Hospital, Limoges, France.
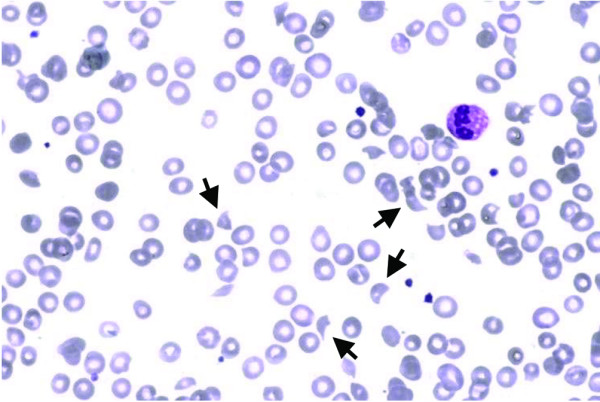
Blood smear from a patient with thrombocytopenic thrombotic purpura, due to deficiency of ADAMTS-13. The arrows indicate schistocytes generated by mechanical damage to red cells. Also note the reduced number of platelets, indicating thrombocytopenia. Giemsa staining, ×40. Courtesy of Dr J van der Lelie, Academic Medical Center, Amsterdam, the Netherlands.
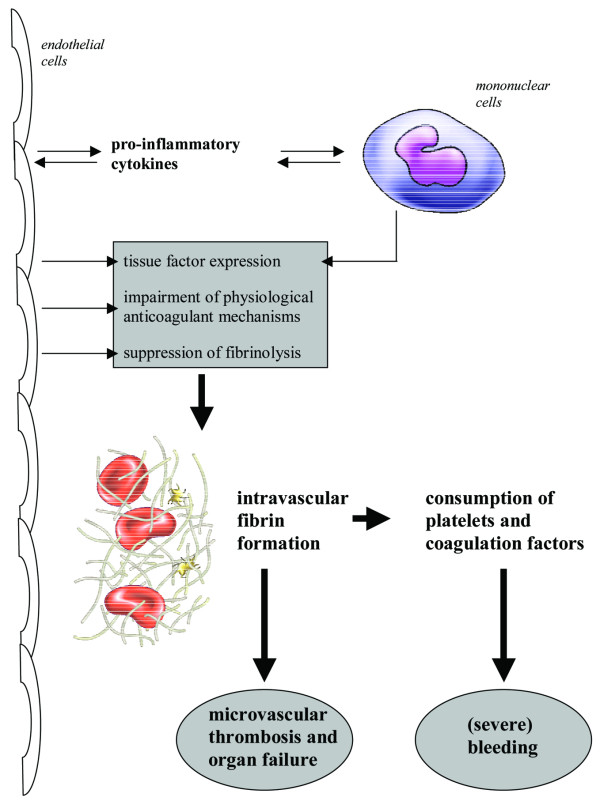
Schematic representation of the systemic activation of coagulation during a severe inflammatory response. Pro-inflammatory cytokines activate mononuclear cells and endothelial cells (which thereupon can also produce cytokines). Mononuclear cells and endothelial cells express tissue factor, the main initiator of coagulation. Simultaneously, impairment of the physiological anticoagulant mechanism and endogenous fibrinolysis, due to down-regulation of endothelial-bound proteins and endothelial cell perturbation, cause an insufficient counterbalance towards intravascular fibrin formation, which may contribute to organ failure. Simultaneously, consumption of platelets and clotting factors may cause serious bleeding.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
