

Reducing the impact of the next influenza pandemic using household-based public health interventions
- PMID: 16881729
- PMCID: PMC1526768
- DOI: 10.1371/journal.pmed.0030361
Reducing the impact of the next influenza pandemic using household-based public health interventions
Abstract
Background: The outbreak of highly pathogenic H5N1 influenza in domestic poultry and wild birds has caused global concern over the possible evolution of a novel human strain [1]. If such a strain emerges, and is not controlled at source [2,3], a pandemic is likely to result. Health policy in most countries will then be focused on reducing morbidity and mortality.
Methods and findings: We estimate the expected reduction in primary attack rates for different household-based interventions using a mathematical model of influenza transmission within and between households. We show that, for lower transmissibility strains [2,4], the combination of household-based quarantine, isolation of cases outside the household, and targeted prophylactic use of anti-virals will be highly effective and likely feasible across a range of plausible transmission scenarios. For example, for a basic reproductive number (the average number of people infected by a typically infectious individual in an otherwise susceptible population) of 1.8, assuming only 50% compliance, this combination could reduce the infection (symptomatic) attack rate from 74% (49%) to 40% (27%), requiring peak quarantine and isolation levels of 6.2% and 0.8% of the population, respectively, and an overall anti-viral stockpile of 3.9 doses per member of the population. Although contact tracing may be additionally effective, the resources required make it impractical in most scenarios.
Conclusions: National influenza pandemic preparedness plans currently focus on reducing the impact associated with a constant attack rate, rather than on reducing transmission. Our findings suggest that the additional benefits and resource requirements of household-based interventions in reducing average levels of transmission should also be considered, even when expected levels of compliance are only moderate.
Conflict of interest statement
Figures



 , the average number of secondary cases generated by an individual chosen at random in an otherwise susceptible population:
, the average number of secondary cases generated by an individual chosen at random in an otherwise susceptible population:  (see Figure S3).
(see Figure S3).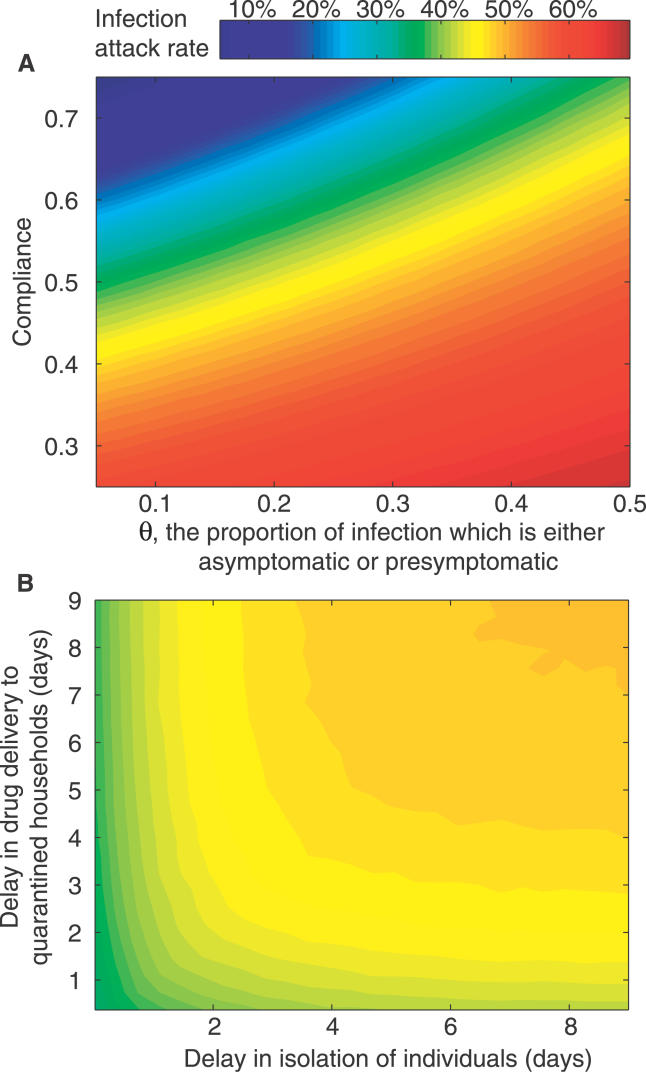
References
-
- Clayton J. Looming flu pandemic has experts crying fowl. Nat Med. 2003;9:375. - PubMed
-
- Ferguson NM, Cummings DAT, Cauchemez S, Fraser C, Riley S, et al. Strategies for containing an emerging influenza pandemic in Southeast Asia. Nature. 2005;437:209–214. - PubMed
-
- Longini IM, Nizam A, Xu SF, Ungchusak K, Hanshaoworakul W, et al. Containing pandemic influenza at the source. Science. 2005;309:1083–1087. - PubMed
-
- Heesterbeek JAP. A brief history of R-0 and a recipe for its calculation. Acta Biotheor. 2002;50:189–204. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
