

Nicotine replacement therapy for long-term smoking cessation: a meta-analysis
- PMID: 16885576
- PMCID: PMC2563611
- DOI: 10.1136/tc.2005.015487
Nicotine replacement therapy for long-term smoking cessation: a meta-analysis
Abstract
Objective: To assess if the effect of a single treatment episode with nicotine replacement therapy (NRT) enhances smoking cessation over many years.
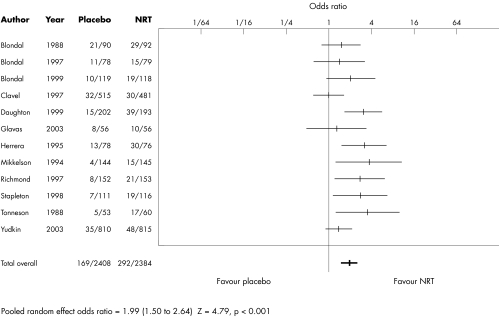
Data sources: Meta-analysis of all randomised controlled trials of NRT with final follow-up more than one year after the start of treatment. Twelve eligible trials were identified, all placebo-controlled, having final follow-ups ranging from 2-8 years. All had earlier follow-ups at 12 months. They comprised 2408 active and 2384 placebo treatment participants.
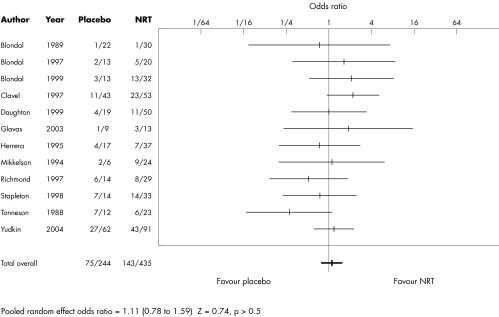
Data synthesis: The odds ratio (OR) in favour of NRT at final follow-up was 1.99 (95% confidence interval (CI) 1.50 to 2.64). There was no evidence that the effect varied according to length of final follow-up (beta = 0.92, p = 0.28) or duration of initial NRT treatment (beta = 0.99, p > 0.5). The overall relapse rate between the 12 months and final follow-up was 30.0% (95% CI 23.5% to 37.5%). This rate did not differ between NRT and control groups (OR 1.11, 95% CI 0.78 to 1.59), or length of initial NRT treatment. There was also no evidence that it varied according to length of final follow up. Due to relapse, the overall efficacy of NRT treatment in terms of additional ex-smokers declined from 10.7% over and above placebo (6.6% to 14.8%) after one year to 7.2% (3.8% to 11.3%) at an average of 4.3 years follow up.
Conclusions: The relative efficacy of a single course of NRT remains constant over many years. The majority of relapse after 12 months occurs within the first or second year and is not detectable thereafter, suggesting that NRT has a permanent effect on smoking cessation. However, initial relapse after one year has the effect of diminishing the number of ex-smokers that can be ultimately attributed to NRT. Results after only 6-12 months of follow-up, as used in existing reviews and treatment guidelines, will overestimate the lifetime benefit and cost-efficacy of NRT by about 30%. Because the long-term benefit of NRT is modest, tobacco dependence treatment might be better viewed as a chronic disorder, requiring repeated episodes of treatment.
Conflict of interest statement
Competing interest statement: JFE has been reimbursed by manufacturers of nicotine replacement products for attending international conferences and to give lectures on smoking cessation. The Institute of Social and Preventive Medicine of the University of Geneva has received grants from Novartis and Pfizer to develop computer‐tailored smoking cessation counselling programs, led by JFE. JS has acted as an adviser to several organisations with an interest in smoking cessation, including manufacturers of nicotine replacement products, for which he has received remuneration. He has also conducted a number of Medial Research Council funded clinical trials that also received support from the manufacturers of nicotine replacement products.
References
-
- Anthonisen N, Skeins A, Wise R.et al The effects of a smoking cessation intervention on 14. 5‐year mortality: a randomized clinical trial, Ann Intern Med 2005142233–239. - PubMed
-
- Silagy C, Lancaster T, Stead L.et alNicotine replacement therapy for smoking cessation. The Cochrane Library, Issue 1, 2005. Chichester, UK: John Wiley & Sons, Ltd,
-
- Fiore M C, Baily W C, Cohen S J.et alTreating tobacco use and dependence. Clinical Practice Guideline. Rockville, Maryland: US Department of Health and Human Services, Public Health Service. June 2000
-
- US Department of Health and Human Services The health benefits of smoking cessation. A report of the Surgeon General, 1990. Rockville, Maryland: Public Health Service, Centers for Disease Control, Office on Smoking and Health, 1990, (DHHS Publication No (CDC) 90‐8416. )
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical