

The association of newly identified respiratory viruses with lower respiratory tract infections in Korean children, 2000-2005
- PMID: 16886150
- PMCID: PMC7107986
- DOI: 10.1086/506350
The association of newly identified respiratory viruses with lower respiratory tract infections in Korean children, 2000-2005
Abstract
Background: This study was performed to evaluate the associations of newly recognized viruses, namely, human metapneumovirus (hMPV), human coronavirus (HCoV)-NL63, and human bocavirus (HBoV) with lower respiratory tract infections (LRTIs) in previously healthy children.
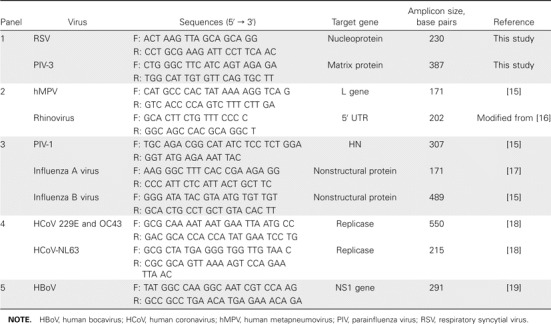
Methods: To determine the prevalences of 11 viruses--respiratory syncytial virus (RSV), adenovirus, rhinovirus, parainfluenza viruses (PIVs) 1 and 3, influenza viruses A and B, hMPV, HCoV, HCoV-NL63, and HBoV--among infants or children with LRTIs, in association with their epidemiologic characteristics, we performed multiplex reverse-transcriptase polymerase chain reaction on nasopharyngeal aspirates obtained from 515 children < or =5 years old with LRTIs during the period 2000-2005.
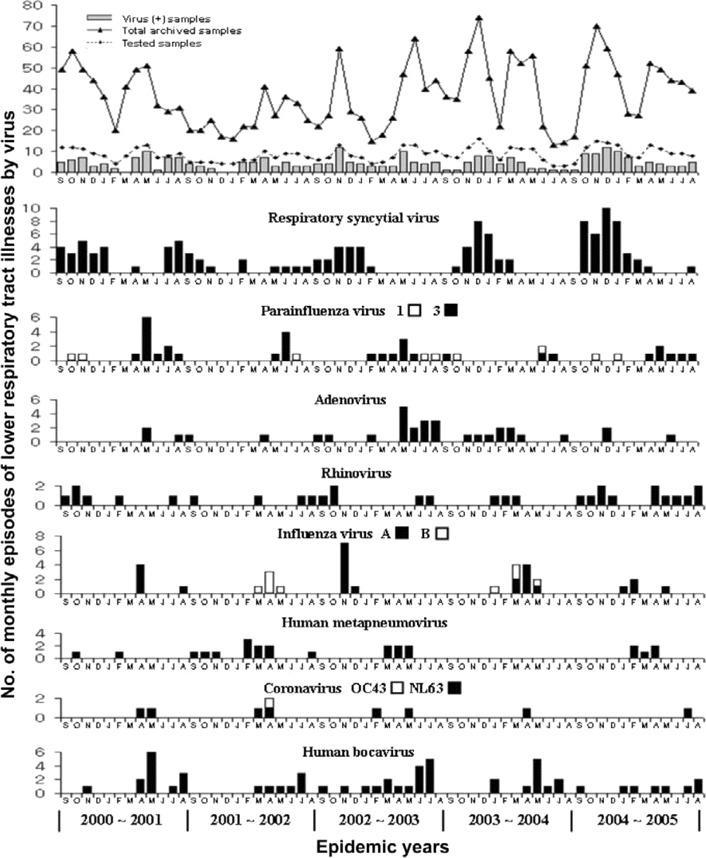
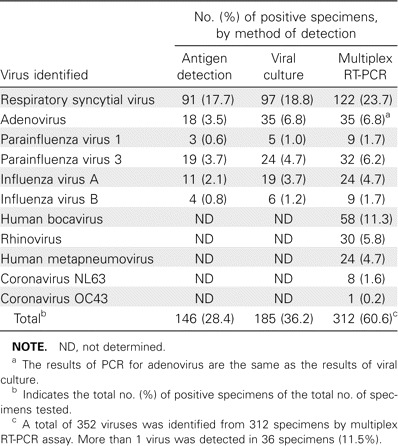
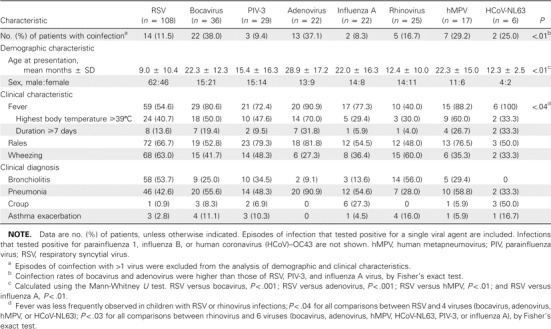
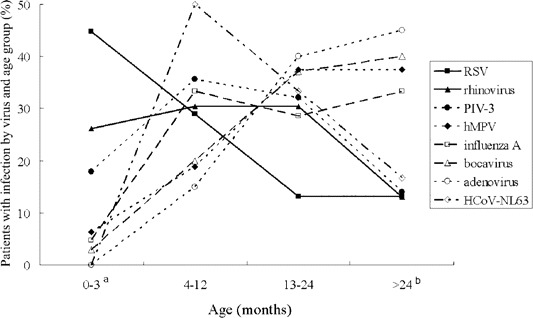
Results: Viruses were identified in 312 (60.6%) of the 515 patients. RSV was detected in 122 (23.7%), HBoV in 58 (11.3%), adenovirus in 35 (6.8%), PIV-3 in 32 (6.2%), rhinovirus in 30 (5.8%), hMPV in 24 (4.7%), influenza A in 24 (4.7%), PIV-1 in 9 (1.7%), influenza B in 9 (1.7%), and HCoV-NL63 in 8 (1.6%). Coinfections with > or =2 viruses were observed in 36 patients (11.5%). Twenty-two patients (37.9%) infected with HBoV had a coinfection. Bronchiolitis was frequently diagnosed in patients who tested positive for RSV, PIV-3, or rhinovirus, whereas influenza A, PIV-1, and HCoV-NL63 were commonly found in patients with croup. The age distributions of patients with viral infections differed; notably, RSV was responsible for 77% of LRTIs that occurred in infants < or =3 months old. The number of hMPV infections peaked between February and April, whereas the number of HCoV-NL63 infections peaked between April and May.
Conclusions: This study describes the features of LRTIs associated with newly identified viruses in children, compared with those associated with known viruses. Additional investigations are required to define the role of HBoV in LRTI.
Figures
References
-
- Henderson FW, Clyde WA, Jr, Collier AM, et al. The etiologic and epidemiologic spectrum of bronchiolitis in pediatric practice. J Pediatr. 1979;95:183–90. - PubMed
-
- Hall CB, Walsh EE, Schnabel KC, et al. Occurrence of groups A and B of respiratory syncytial virus over 15 years: associated epidemiologic and clinical characteristics in hospitalized and ambulatory children. J Infect Dis. 1990;162:1283–90. - PubMed
-
- Yun BY, Kim MR, Park JY, Choi EH, Lee HJ, Yun CK. Viral etiology and epidemiology of acute lower respiratory tract infections in Korean children. Pediatr Infect Dis J. 1995;14:1054–9. - PubMed
-
- Hong JY, Lee HJ, Piedra PA, et al. Lower respiratory tract infections due to adenovirus in hospitalized Korean children: epidemiology, clinical features, and prognosis. Clin Infect Dis. 2001;32:1423–9. - PubMed
-
- Papadopoulos NG, Moustaki M, Tsolia M, et al. Association of rhinovirus infection with increased disease severity in acute bronchiolitis. Am J Respir Crit Care Med. 2002;165:1285–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
