

GH peak response to GHRH-arginine: relationship to insulin resistance and other cardiovascular risk factors in a population of adults aged 50-90
- PMID: 16886956
- PMCID: PMC1618818
- DOI: 10.1111/j.1365-2265.2006.02569.x
GH peak response to GHRH-arginine: relationship to insulin resistance and other cardiovascular risk factors in a population of adults aged 50-90
Abstract
Objective: To assess the GH response to GHRH-arginine in apparently healthy adults in relation to cardiovascular risk factors.
Design: Cross-sectional.
Patients: Eighty-six male and female volunteers aged 50-90.
Measurements: GH peak response to GHRH-arginine and cardiovascular risk factors, including obesity, insulin resistance, low levels of high density lipoprotein (HDL) cholesterol, elevated triglycerides, and hypertension. The primary outcome measurement was GH response to GHRH-arginine. The relationship between GH peak responses and cardiovascular risk factors was determined after data collection.
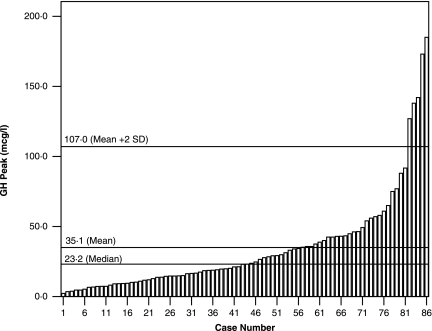
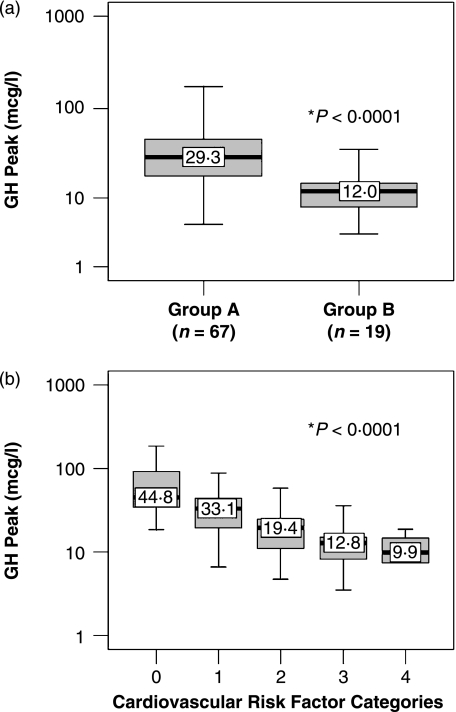
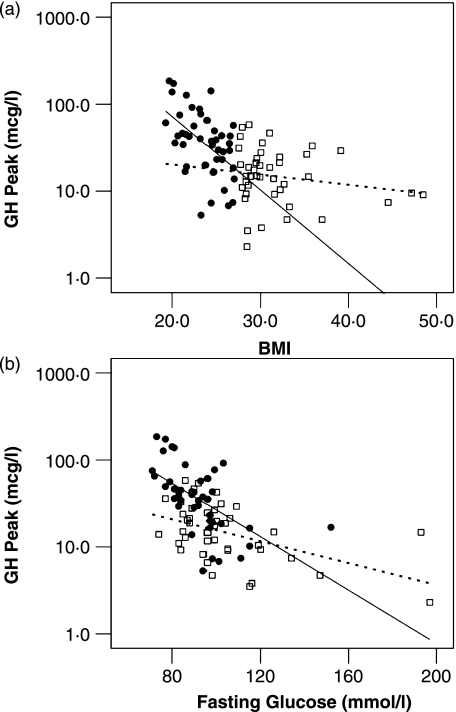
Results: GH peaks were highly variable, ranging from 2.3 to 185 microg/l (14% with GH peaks < 9 microg/l). An increasing number of cardiovascular risk factors were associated with a lower mean GH peak (P < 0.0001). By univariate analysis, fasting glucose, insulin, body mass index (BMI), HDL cholesterol and triglycerides were significantly associated with GH peak (all P < 0.0001). Multiple regression analysis revealed that fasting glucose, fasting insulin, BMI, triglycerides and sex accounted for 54% of GH peak variability. The role of abdominal fat as it relates to GH peak was explored in a subset of 45 subjects. Trunk fat and abdominal subregion fat measured by dual energy X-ray absorptiometry (DXA) were inversely related to GH peak (P < 0.008 and 0.001, respectively). Analysis of this subgroup by multiple regression revealed that subregion abdominal fat became the significant obesity-related determinant of GH peak, but still lagged behind fasting insulin and glucose.
Conclusions: GH response to secretagogues was highly variable in apparently healthy adults aged 50-90 years. Peak GH was significantly related to fasting glucose, insulin, BMI, HDL cholesterol, triglycerides, trunk fat and abdominal subregion fat, with fasting glucose ranking first by multiple regression analysis. There was a strong relationship between cardiovascular risk factors and low GH, with individual risk factors being additive. Although these data do not differentiate between low GH being a cause or an effect of these cardiovascular risk factors, they indicate that the relationship between low GH and increased cardiovascular risk may be physiologically important in the absence of pituitary disease.
Figures
References
-
- Reaven GM. Insulin resistance/compensatory hyperinsulinemia, essential hypertension, and cardiovascular disease. Journal of Clinical Endocrinology and Metabolism. 2003;88:2399–2403. - PubMed
-
- Isomaa B, Almgren P, Tuomi T, Forsen B, Lahti K, Nissen M, Taskinen MR, Groop L. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care. 2001;24:683–689. - PubMed
-
- Newman CB, Kleinberg DL. Adult growth hormone deficiency. Endocrinologist. 1998;8:178–186.
-
- de Boer H, Blok GJ, van der Veen EA. Clinical aspects of growth hormone deficiency in adults. ENDO Review. 1995;16:63–86. - PubMed
-
- Markussis V, Beshyah SA, Fisher C, Sharp P, Nicolaides AN, Johnston DG. Detection of premature atherosclerosis by high-resolution ultrasonography in symptom-free hypopituitary adults. Lancet. 1992;340:1188–1192. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
