

Medial temporal atrophy but not memory deficit predicts progression to dementia in patients with mild cognitive impairment
- PMID: 16891386
- PMCID: PMC2077364
- DOI: 10.1136/jnnp.2005.082651
Medial temporal atrophy but not memory deficit predicts progression to dementia in patients with mild cognitive impairment
Abstract
Background: The diagnosis of mild cognitive impairment (MCI) is clinically unhelpful, as many patients with MCI develop dementia but many do not.
Objective: To identify clinical instruments easily applicable in the clinical routine that might be useful to predict progression to dementia in patients with MCI assessed in the outpatient facility of a memory clinic.
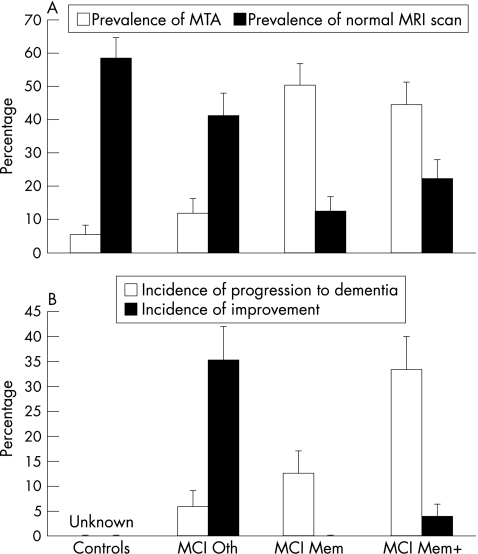
Participants and methods: 52 dementia-free patients (mean (standard deviation) age 70 (6) years; 56% women) with MCI, and 65 healthy controls (age 69 (6) years; 54% women) underwent brain magnetic resonance scan with standardised visual assessment of medial temporal atrophy (MTA) and subcortical cerebrovascular lesions (SVLs). Follow-up assessment occurred 15.4 (SD 3.4) months after baseline to detect incident dementia and improvement, defined as normal neuropsychological performance on follow-up.
Results: Patients were classified into three groups according to the presence of memory disturbance only (MCI Mem), other neuropsychological deficits (MCI Oth) or both (MCI Mem+). MCI Mem and Mem+ showed MTA more frequently (31% and 47% v 5% and 14% of controls and MCI Oth, p<0.001). 11 patients developed dementia (annual rate 16.5%) and 7 improved on follow-up. The only independent predictor of progression was MTA (odds ratio (OR) 7.1, 95% confidence interval (CI) 1.4 to 35.0), whereas predictors of improvement were the absence of memory impairment (OR 18.5, 95% CI 2.0 to 171.3) and normal MRI scan (OR 10.0, 95% CI 1.7 to 60.2).
Conclusion: Neuropsychological patterns identify groups of patients with MCI showing specific clinical features and risk of progression to dementia. MTA clinically rated with a visual scale is the most relevant predictor of progression and improvement.
Conflict of interest statement
Competing interests: None declared.
References
-
- Petersen R C, Doody R, Kurz A.et al Current concepts in mild cognitive impairment. Arch Neurol 2001581985–1992. - PubMed
-
- Bennett D A, Wilson R S, Schneider J A.et al Natural history of mild cognitive impairment in older persons. Neurology 200259198–205. - PubMed
-
- Frisoni G B, Padovani A, Wahlund L O. The predementia diagnosis of Alzheimer disease. Alzheimer Dis Assoc Disord 20041851–55. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical