

Exposure of neonates to respiratory syncytial virus is critical in determining subsequent airway response in adults
- PMID: 16893457
- PMCID: PMC1563465
- DOI: 10.1186/1465-9921-7-107
Exposure of neonates to respiratory syncytial virus is critical in determining subsequent airway response in adults
Abstract
Background: Respiratory syncytial virus (RSV) is the most common cause of acute bronchiolitis in infants and the elderly. Furthermore, epidemiological data suggest that RSV infection during infancy is a potent trigger of subsequent wheeze and asthma development. However, the mechanism by which RSV contributes to asthma is complex and remains largely unknown. A recent study indicates that the age of initial RSV infection is a key factor in determining airway response to RSV rechallenge. We hypothesized that severe RSV infection during neonatal development significantly alters lung structure and the pulmonary immune micro-environment; and thus, neonatal RSV infection is crucial in the development of or predisposition to allergic inflammatory diseases such as asthma.
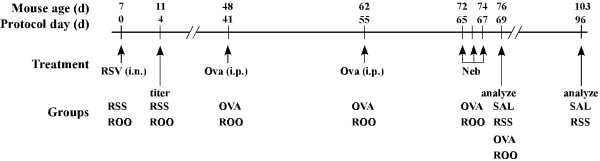
Methods: To investigate this hypothesis the present study was conducted in a neonatal mouse model of RSV-induced pulmonary inflammation and airway dysfunction. Seven-day-old mice were infected with RSV (2 x 10(5) TCID50/g body weight) and allowed to mature to adulthood. To determine if neonatal RSV infection predisposed adult animals to enhanced pathophysiological responses to allergens, these mice were then sensitized and challenged with ovalbumin. Various endpoints including lung function, histopathology, cytokine production, and cellularity in bronchoalveolar lavage were examined.
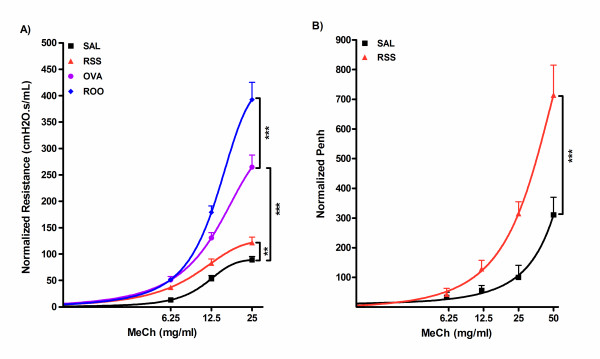
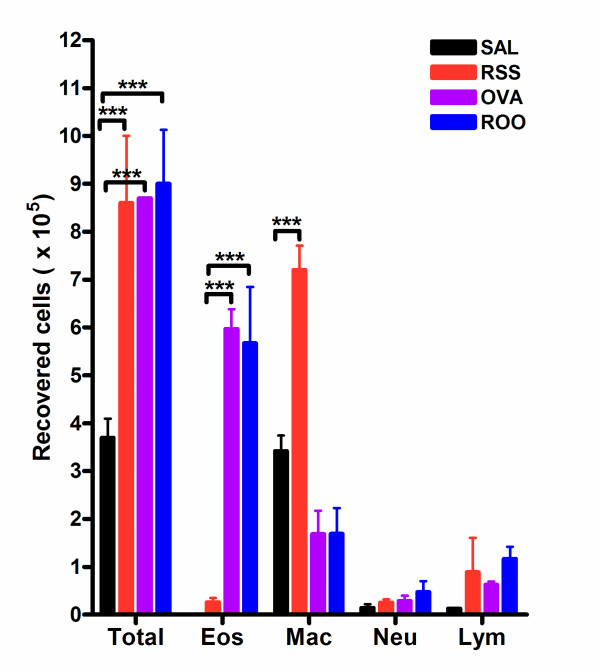
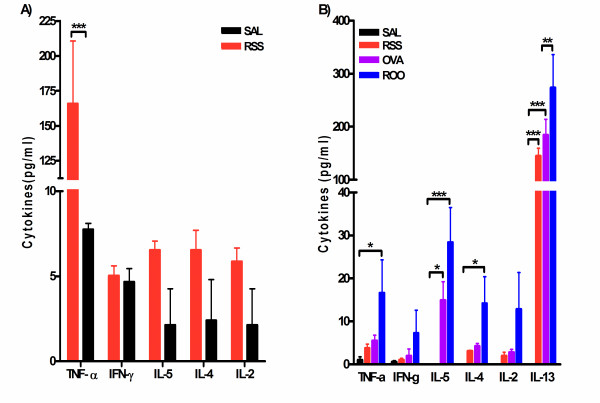
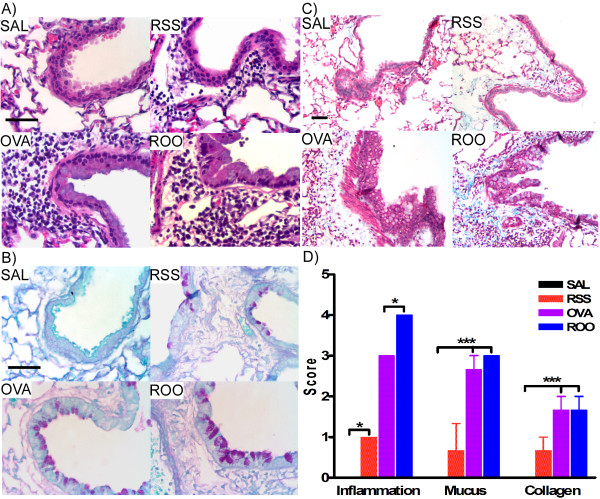
Results: RSV infection in neonates alone led to inflammatory airway disease characterized by airway hyperreactivity, peribronchial and perivascular inflammation, and subepithelial fibrosis in adults. If early RSV infection was followed by allergen exposure, this pulmonary phenotype was exacerbated. The initial response to neonatal RSV infection resulted in increased TNF-alpha levels in bronchoalveolar lavage. Interestingly, increased levels of IL-13 and mucus hyperproduction were observed almost three months after the initial infection with RSV.
Conclusion: Neonatal RSV exposure results in long term pulmonary inflammation and exacerbates allergic airways disease. The early increase in TNF-alpha in the bronchoalveolar lavage implicates this inflammatory cytokine in orchestrating these events. Finally, the data presented emphasize IL-13 and TNF-alpha as potential therapeutic targets for treating RSV induced-asthma.
Figures
Similar articles
-
Building a better neonatal mouse model to understand infant respiratory syncytial virus disease.Respir Res. 2015 Aug 1;16(1):91. doi: 10.1186/s12931-015-0244-0. Respir Res. 2015. PMID: 26231396 Free PMC article.
-
A role for airway remodeling during respiratory syncytial virus infection.Respir Res. 2005 Oct 21;6(1):122. doi: 10.1186/1465-9921-6-122. Respir Res. 2005. PMID: 16242038 Free PMC article.
-
[Combined effects of neonatal Bacillus Calmette-Guerin vaccination and respiratory syncytial infection on experimental asthma in mice].Zhonghua Er Ke Za Zhi. 2006 Jun;44(6):420-4. Zhonghua Er Ke Za Zhi. 2006. PMID: 16836848 Chinese.
-
[Respiratory syncytial virus infection and asthma].Allergol Immunopathol (Madr). 2001 May-Jun;29(3):140-6. doi: 10.1016/s0301-0546(01)79034-9. Allergol Immunopathol (Madr). 2001. PMID: 11434889 Review. Spanish.
-
Contribution of neuroimmune mechanisms to airway inflammation and remodeling during and after respiratory syncytial virus infection.Pediatr Infect Dis J. 2003 Feb;22(2 Suppl):S66-74; discussion S74-5. doi: 10.1097/01.inf.0000053888.67311.1d. Pediatr Infect Dis J. 2003. PMID: 12671455 Review.
Cited by
-
Toward primary prevention of asthma. Reviewing the evidence for early-life respiratory viral infections as modifiable risk factors to prevent childhood asthma.Am J Respir Crit Care Med. 2015 Jan 1;191(1):34-44. doi: 10.1164/rccm.201405-0901PP. Am J Respir Crit Care Med. 2015. PMID: 25369458 Free PMC article. Review.
-
Respiratory Syncytial Virus Disease Is Mediated by Age-Variable IL-33.PLoS Pathog. 2015 Oct 16;11(10):e1005217. doi: 10.1371/journal.ppat.1005217. eCollection 2015 Oct. PLoS Pathog. 2015. PMID: 26473724 Free PMC article.
-
IL-4Rα on CD4+ T cells plays a pathogenic role in respiratory syncytial virus reinfection in mice infected initially as neonates.J Leukoc Biol. 2013 Jun;93(6):933-42. doi: 10.1189/jlb.1012498. Epub 2013 Mar 29. J Leukoc Biol. 2013. PMID: 23543769 Free PMC article.
-
The fusion protein of respiratory syncytial virus triggers p53-dependent apoptosis.J Virol. 2008 Apr;82(7):3236-49. doi: 10.1128/JVI.01887-07. Epub 2008 Jan 23. J Virol. 2008. PMID: 18216092 Free PMC article.
-
The human side of influenza.J Leukoc Biol. 2012 Jul;92(1):83-96. doi: 10.1189/jlb.1011506. Epub 2012 Feb 23. J Leukoc Biol. 2012. PMID: 22362872 Free PMC article. Review.
References
-
- McConnochie KM, Roghmann KJ. Bronchiolitis as a possible cause of wheezing in childhood: new evidence. Pediatrics. 1984;74(1):1–10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
