

Sensemaking of patient safety risks and hazards
- PMID: 16898979
- PMCID: PMC1955349
- DOI: 10.1111/j.1475-6773.2006.00565.x
Sensemaking of patient safety risks and hazards
Abstract
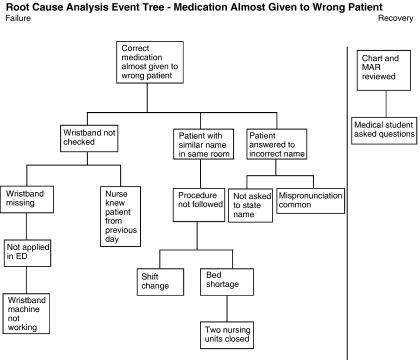
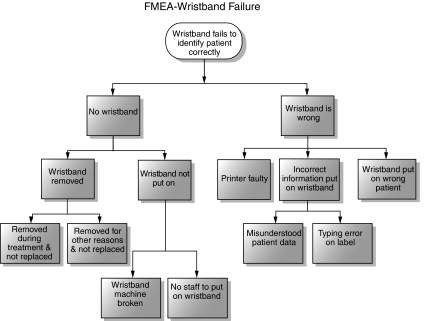
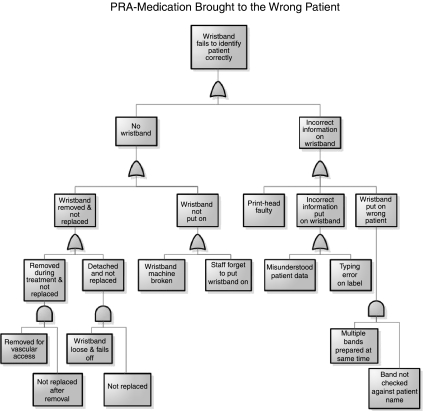
In order for organizations to become learning organizations, they must make sense of their environment and learn from safety events. Sensemaking, as described by Weick (1995), literally means making sense of events. The ultimate goal of sensemaking is to build the understanding that can inform and direct actions to eliminate risk and hazards that are a threat to patient safety. True sensemaking in patient safety must use both retrospective and prospective approach to learning. Sensemaking is as an essential part of the design process leading to risk informed design. Sensemaking serves as a conceptual framework to bring together well established approaches to assessment of risk and hazards: (1) at the single event level using root cause analysis (RCA), (2) at the processes level using failure modes effects analysis (FMEA) and (3) at the system level using probabilistic risk assessment (PRA). The results of these separate or combined approaches are most effective when end users in conversation-based meetings add their expertise and knowledge to the data produced by the RCA, FMEA, and/or PRA in order to make sense of the risks and hazards. Without ownership engendered by such conversations, the possibility of effective action to eliminate or minimize them is greatly reduced.
Figures
References
-
- Aspden PJM, Wolcott CorriganJ, Erickson SM, editors. Patient Safety: Achieving a New Standard of Care. Washington, DC: The National Academies Press; 2004. - PubMed
-
- Battles JB, Kanki BG. The Use of Scio-Technical Probabilistic Risk Assessment at AHRQ and NASA. In: Spitzer C, Schmocker U, Dang VN, editors. Probabilistic Safety Assessment and Management 2004. Vol. 4. Berlin: Springer; 2004. pp. 2212–7.
-
- Battles JB, Kaplan HS, Van der Schaaf TW, Shea CE. The Attributes of Medical Event-Reporting Systems: Experience with a Prototype Medical Event-Reporting System for Transfusion Medicine. Archives of Pathology and Laboratory Medicine. 1998;122(3):231–8. - PubMed
-
- Battles JB, Shea CE. A System of Analyzing Medical Errors to Improve GME Curricula and Programs. Academic Medicine. 2001;76(2):125–33. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
