

Enterogenesis in a clinically feasible model of mechanical small-bowel lengthening
- PMID: 16904972
- PMCID: PMC1764912
- DOI: 10.1016/j.surg.2006.03.005
Enterogenesis in a clinically feasible model of mechanical small-bowel lengthening
Abstract
Background: Recent work indicates that mechanical force induces small-bowel growth, although methods reported do not have direct clinical application. We report a clinically feasible technique of enterogenesis and describe intestinal function in this model.
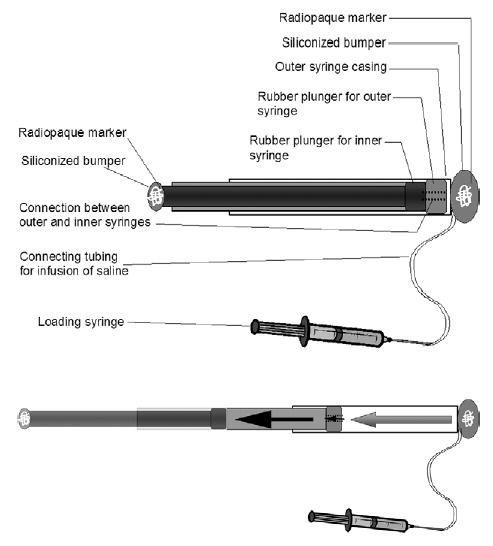
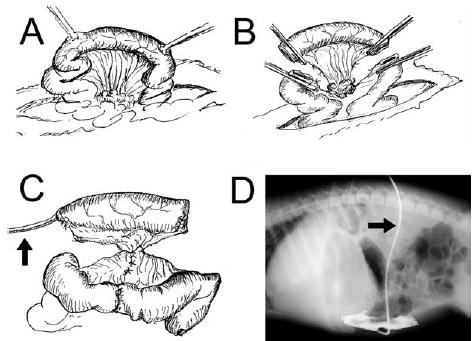
Methods: Using a pig model (n = 11), we stretched isolated small intestinal segments mechanically for 7 days in vivo with an intraluminal device. Control segments were not stretched. Morphology, histology, and epithelial proliferation were assessed. Absorption and epithelial barrier function were examined in an Ussing chamber.
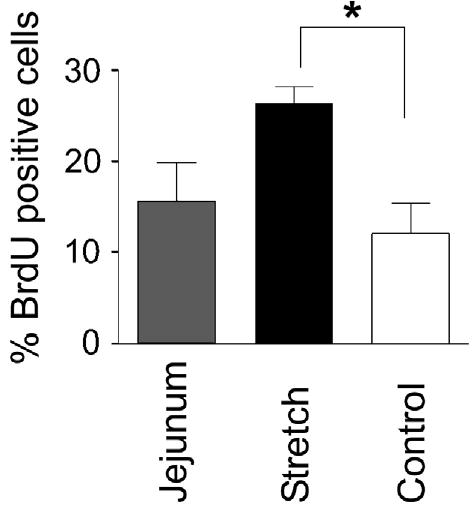
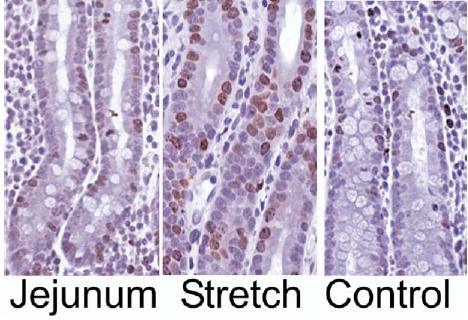
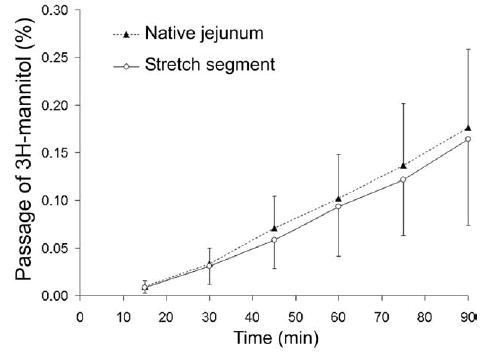
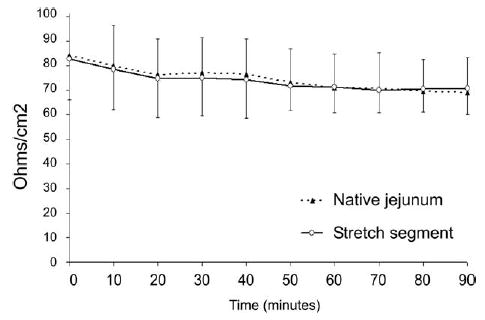
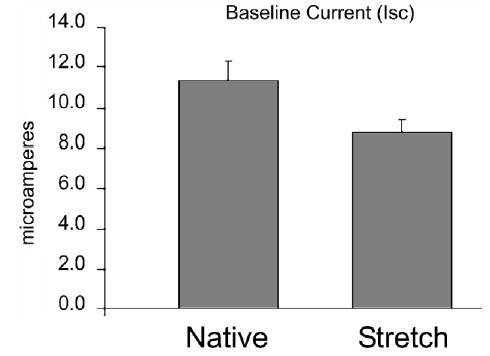
Results: Stretch segments were significantly longer than Control segments and had nearly 2-fold greater surface area (P < .001). Mucosal thickness was much greater in Stretch than Control segments (772 +/- 134 vs. 647 +/- 75 microm, P = .02). Although villus height was reduced in Stretch and Control segments (353 +/- 76 vs. 324 +/- 76 microm, P = .6) versus native jejunum (522 +/- 87, P < .0005), crypt depth was increased dramatically in Stretch (450 +/- 95 microm) versus Control segments (341 +/- 64, P = .005). This observation was accompanied by a 2-fold increase in cellular proliferation (26.3 +/- 3.8 vs 12.1 +/- 6.6 % bromodeoxyuridine+, P < .05). Barrier function was intact ([3H]-mannitol permeation, 0.16 +/- 0.08%, vs native jejunum, 0.17 +/- 0.08%, P = .81). Glucose-mediated sodium transport was similar in Stretch versus native jejunum segments (60.0 +/- 23.5 vs 82.3 +/- 47.3 microA/cm2, P = .31), as was carbachol-induced chloride transport (82.4 +/- 72.2 vs 57.2 +/- 33.4 microA/cm2, P = .54) and alanine absorption (16.46 +/- 12.94 vs 23.53 +/- 21.31 microA/cm2, P = .53).
Conclusions: Mechanical stretching induces small intestinal growth, while maintaining function. Epithelial architecture does change, such that a decrease in villus height is offset by a marked increase in crypt depth and a 2-fold increase in epithelial proliferation. Epithelial barrier and absorptive functions remain intact. The device described may have direct clinical applicability.
Figures
References
-
- Warner BW, Ziegler MM. Management of the short bowel syndrome in the pediatric population. Pediatr Clin North Am. 1993;40(6):1335–50. - PubMed
-
- Barksdale EM, Stanford A. The surgical management of short bowel syndrome. Curr Gastroenterol Rep. 2002;4(3):229–37. - PubMed
-
- Vanderhoof JA. Short bowel syndrome in children. Curr Opin Pediatr. 1995;7(5):560–8. - PubMed
-
- Messing B, Crenn P, Beau P, et al. Long-term survival and parenteral nutrition dependence in adult patients with the short bowel syndrome. Gastroenterology. 1999;117(5):1043–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
