

EVALUATION OF DRUG ABUSE TREATMENT MEDICATIONS: CONCORDANCE BETWEEN CLINICAL AND PRECLINICAL STUDIES
Affiliations
- PMID: 16906230
- PMCID: PMC1538975
Item in Clipboard
EVALUATION OF DRUG ABUSE TREATMENT MEDICATIONS: CONCORDANCE BETWEEN CLINICAL AND PRECLINICAL STUDIES
NIDA Res Monogr.
2005 May.
No abstract available
Figures
Cross validation of preclinical and clinical models. Validation of the effectiveness of animal models for preclinical evaluation of drug abuse treatment medications requires assessing the degree of concordance between preclinical studies and outpatient clinical studies. Eventually, the preclinical model should enable users to predict the potential effectiveness of new pharmacotherapies. This interactive process of cross-validation and prediction is essential for refinement of the preclinical model of drug self-administration. From Mello NK (1992); Behavioral Strategies for the Evaluation of New Pharmacotherapies for Drug Abuse Treatment. NIDA Research Monograph 119. Washington, DC: Government Printing Office, pp 150–154.
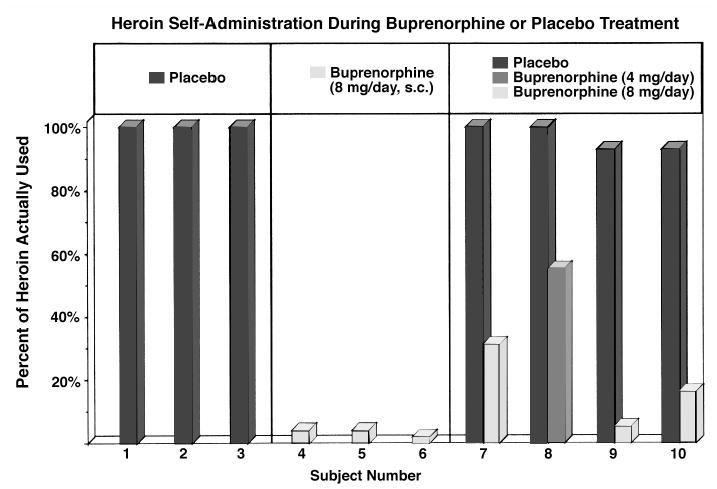
Percentage of available heroin used during 10 days of treatment with buprenorphine or placebo buprenorphine. Three subjects were maintained on placebo-buprenorphine (left columns); three subjects were maintained on buprenorphine (8 mg/day, s.c.) (middle columns), and four subjects were studied under both buprenorphine and placebo-buprenorphine conditions (right columns). Adapted from Mello and Mendelson, Science (1980).
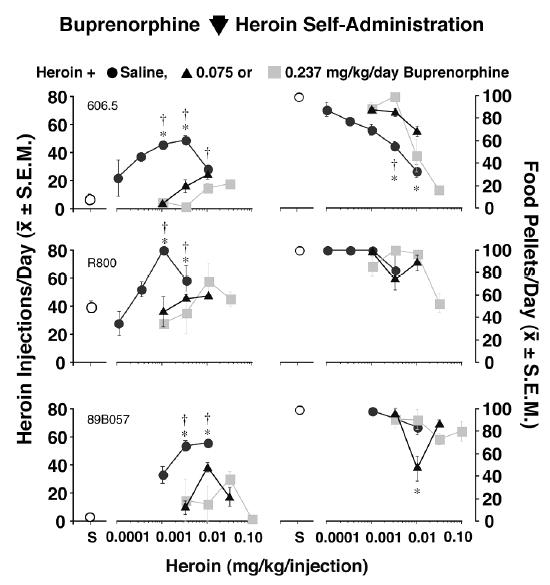
Effects of buprenorphine on heroin and food self-administration in rhesus monkeys. Dose-effect curves for heroin alone (0.0001–0.10 mg/kg/inj) are shown for individual monkeys in the left panel. The mean number of injections per day of heroin during saline treatment (closed circles) or buprenorphine treatment (0.075 mg/kg/day, triangles and 0.237 mg/kg/day, shaded squares) are shown on the left ordinate. Points above S show data from sessions when saline was available for self-administration (open circles). The dose of heroin available for self-administration is shown on the abscissa. In the right panel, food-maintained responding during saline self-administration (open circles) and heroin (0.0001–0.10 mg/kg/inj) self-administration during saline treatment (closed circles) and buprenorphine treatment [0.075 mg/kg/day, triangles and 0.237 mg/kg/day, shaded squares) is shown for individual monkeys. Each data point is the average of the last 3 days of 10 days during saline or buprenorphine treatment (
± S.E.M.). Statistically significant differences between corresponding heroin doses during saline control treatment and buprenorphine treatment are indicated as follows: * 0.075 mg/kg/day buprenorphine different from saline, p<0.05; = = 0.237 mg/kg/day buprenorphine different from saline, p<0.05. Adapted from Mello and Negus, J. Pharmacol. Exp. Ther. (1998).
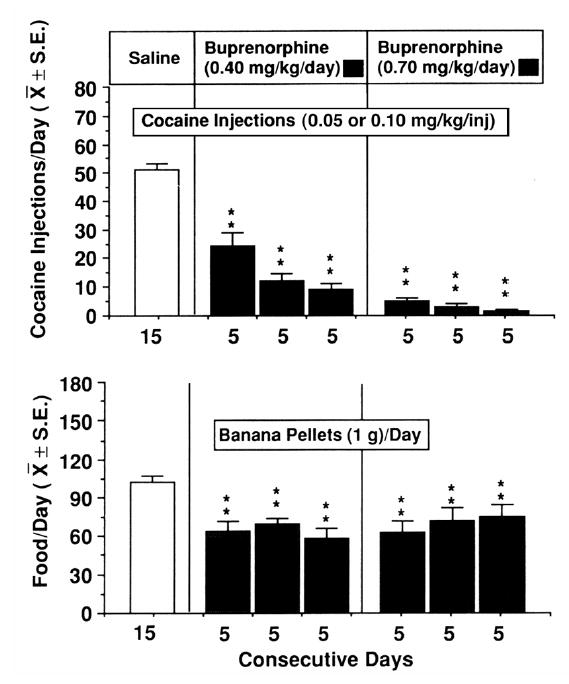
Buprenorphine reduces cocaine self-administration by rhesus monkeys. The effects of single daily infusions of buprenorphine or a saline control solution on cocaine and food self-administration are shown. Saline treatment is shown as an open bar in the left panel and buprenorphine treatment 0.40 mg/kg/day is shown as closed bars in the middle panel and 0.70 mg/kg/day is shown as closed bars in the right panel. The average number of cocaine injections self-administered is shown in the top row. The average number of food pellets self-administered is shown in the second row. The number of days that each treatment condition was in effect is shown on the abscissa. Each data point is the mean ±SEM for five subjects. The statistical significance of each change from the saline treatment as determined by analysis of variance for repeated measures and Dunnett’s tests for multiple comparisons is shown by asterisks (**p< 0.01). Reproduced from Mello et al., Science (1989), with permission of the publishers. Copyright 1989 by the A.A.A.S.
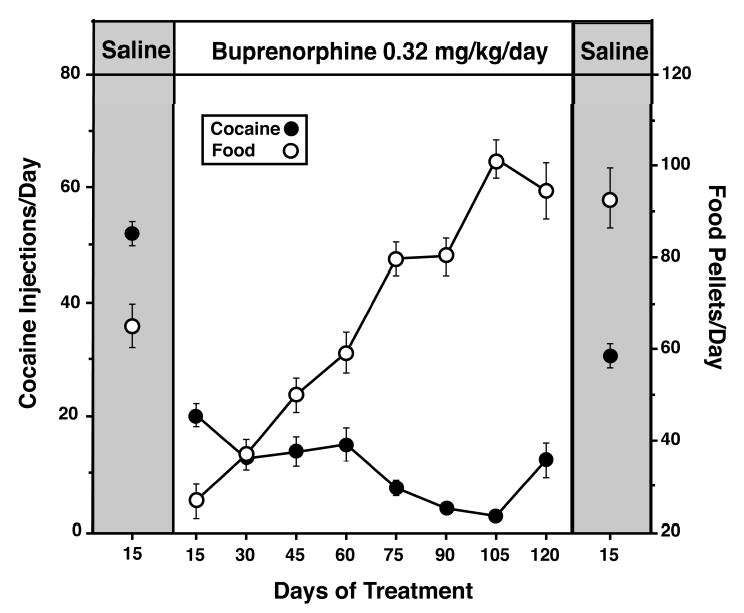
Effects of 3–4 months of daily buprenorphine treatment (0.32 mg/kg/day) on cocaine and food self-administration. Each of the data points for cocaine injections (filled circles) and food pellets (open circles) during the pre-buprenorphine saline control period is the average ±SE of four monkeys over 15 days. The first 100 days of buprenorphine treatment are an average of data from four monkeys and days 101–120 are an average of data from three monkeys. Adapted from Mello et al., J. Pharmacol. Exp. Ther. (1992).
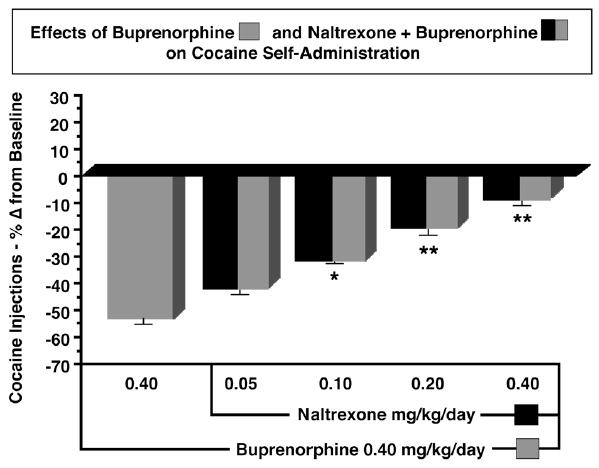
Comparison of the effects of buprenorphine only with buprenorphine-naltrexone combinations on cocaine self-administration. The average number of cocaine injections (mean ±SEM) self-administered are shown as percentage change from the saline treatment baseline before buprenorphine administration. A 10-day period of buprenorphine treatment (0.40 mg/kg/day) is shown at the left as a grey bar. Successive 10-day periods of ascending doses of naltrexone (0.05 – 0.40 mg/kg/day) administered 20 min before buprenorphine (striped and black bars) are shown at the right. Adapted from Mello et al., Neuropsychopharmacology (1993), Macmillan Publishers Ltd.
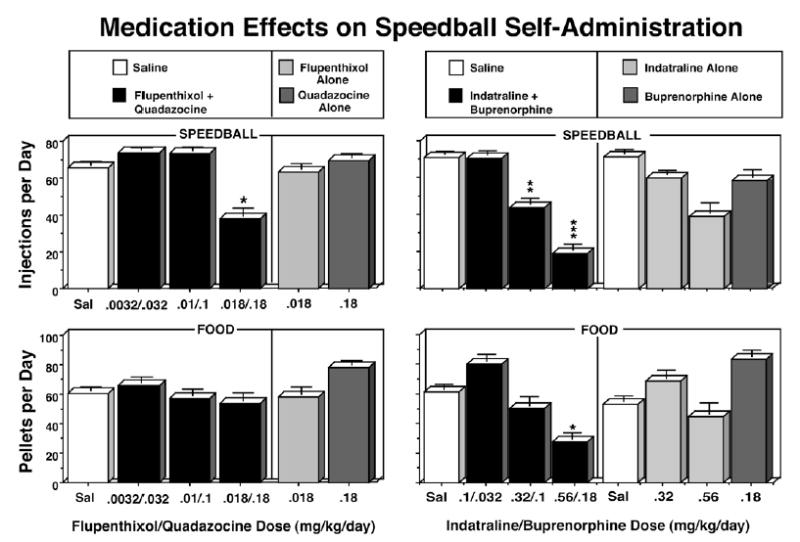
Effects of saline, ascending doses of flupenthixol + quadazocine combinations and flupenthixol or quadazocine alone [left panel] or ascending doses of indatraline + buprenorphine combinations and indatraline or buprenorphine alone on speedball- and food-maintained responding [right panel]. Saline and doses of flupenthixol + quadazocine (mg/kg/day) [left panel] or indatraline + buprenorphine [right panel] are shown on the abscissa. The number of speedball injections per day (row 1) or food pellets per day (row 2) are shown on the left ordinate. Speedballs consisted of a unit dose of cocaine (0.01 mg/kg/inj) and heroin (0.0032 mg/kg/inj) in combination. Speedball- and food-maintained responding during saline treatment are shown as open rectangles, and as black rectangles during treatment with each medication combination. Speedball- and food-maintained responding during treatment with each medication alone are shown as light gray rectangles during treatment with flupenthixol alone [left panel] or indatraline alone [right panel], and as dark gray rectangles during treatment with quadazocine alone [left panel] or buprenorphine alone [right panel]. Each data point represents the average number of injections or food pellets (
± S.E.) during 10 consecutive days of saline or drug treatment in a group of four monkeys [left panel] or three to five monkeys [right panel]. The asterisks indicate a significant change from the saline treatment baseline (*=p<0.05; **=p<0.01; ***=p<0.001). Adapted from Mello and Negus, Neuropsychopharmacology (1999 and 2001), Macmillan Publishers Ltd.
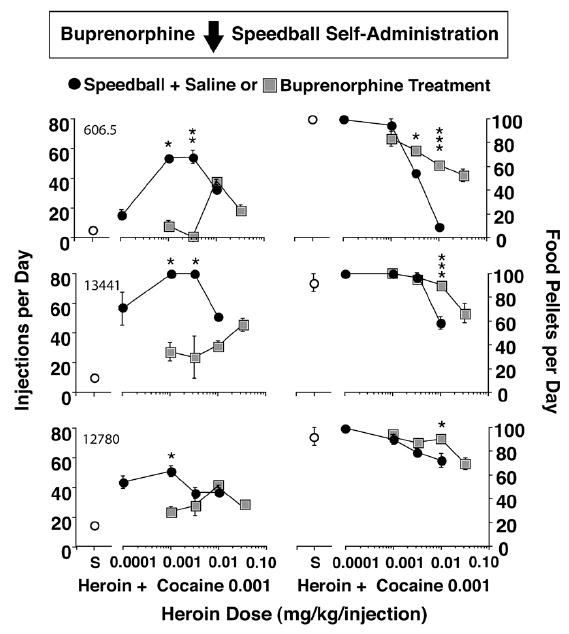
Effects of Buprenorphine (0.237) mg/kg/day on speedball dose-effect curves for individual monkeys. Dose-effect curves for a low dose of cocaine (0.001 mg/kg/inj) in combination with one of four doses of heroin (0.0001–0.032 mg/kg/inj) are shown for individual monkeys (left panel). The unit dose of heroin in combination with cocaine is shown on the abscissa. Points above S show data from saline treatment sessions when saline was the solution available for self-administration (open circles). Self-administration of each heroin + cocaine speedball combination during saline treatment (closed circles) and during buprenorphine treatment (0.237 mg/kg/day) (shaded squares) is shown on the left ordinate as injections per day. Each data point is the average of the last 3 days of 10 days of self-administration of each heroin + cocaine combination for each monkey (
± S.E.M.). Food-maintained responding during saline self-administration (open circles), self-administration of heroin + cocaine combinations during saline treatment (closed circles) and during buprenorphine treatment (0.237 mg/kg/day) (shaded squares) is shown in the right panel. The number of 1g banana-flavored pellets per day earned during each condition is shown on the right ordinate. Statistically significant differences between corresponding speedball doses during saline control treatment and buprenorphine treatment are indicated by asterisks (*=p<0.05; **=p<0.01; ***=p<0.001). From Mello and Negus, J. Pharmacol. Exp. Ther. (1998).
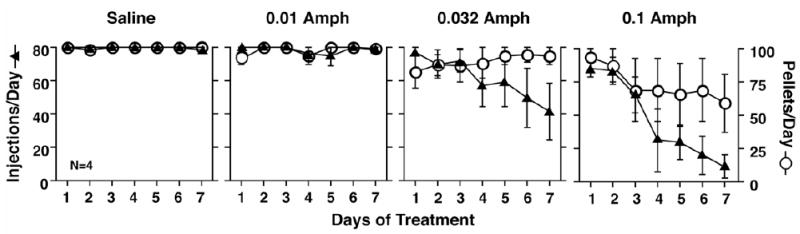
Time course of effects of saline or d-amphetamine (0.01–0.1 mg/kg/hr) on responding for 0.01 mg/kg/injection cocaine and food pellets. Abscissae: Consecutive days of treatment. Left ordinates: Number of cocaine injections (0.01 mg/kg/injection) delivered on each day of treatment (filled triangles, maximum=80). Right ordinates: Number of food pellets delivered on each day of treatment (open circles, maximum=100). Each point shows mean data from four monkeys, and error bars show the SEM. Statistical analysis indicated a significant effect of d-amphetamine dose [F(3,9)=7.93; p=0.0088] and treatment day [F(3,18)=21.96; p<0.0001] on cocaine self-administration and a significant interaction between d-amphetamine dose and treatment day [F(3,54)=4.17; p<0.0001]. A high dose of 0.1 mg/kg/hr d-amphetamine significantly decreased cocaine self-administration relative to saline control (p<0.01, Duncan post hoc test). In contrast, there was not a significant effect of d-amphetamine dose [F(3,9)=2.09; p=0.17] or treatment day [F(3,18)=0.70; p=0.59] on food-maintained responding, although the interaction between d-amphetamine dose and treatment day approached significance [F(3,54)=1.77; p=0.055]. Adapted from Negus and Mello, Drug Alc. Depend. (2003b).
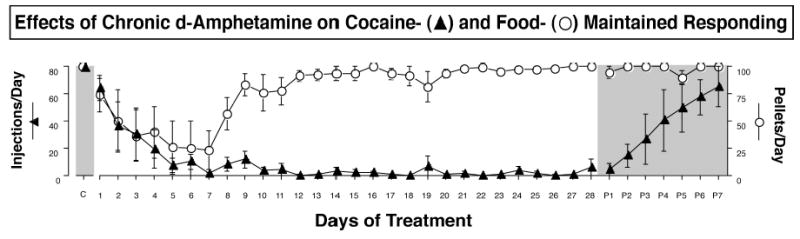
Effects of 28-day treatment with 0.1 mg/kg/hr d-amphetamine on responding for 0.01 mg/kg/injection cocaine and food pellets. Abscissa: Consecutive days of treatment. Left ordinate: Number of cocaine injections (0.01 mg/kg/injection) delivered on each day of treatment (filled triangles, maximum=80). Right ordinate: Number of food pellets delivered on each day of treatment (open circles, maximum=100). Each point shows mean data from four monkeys, and error bars show the SEM. Points in the shaded area on the far left over “C” show average numbers of cocaine injections and food pellets per day when 0.01 mg/kg/injection cocaine was available during saline treatment for 7 days in a separate experiment. Points in the shaded area to the far right over “P1-P7” show post-treatment data collected during the first seven days after d-amphetamine treatment was discontinued. During this time, the same unit dose of cocaine (0.01 mg/kg/injection) was available, and saline was substituted for 0.1 mg/kg/hr d-amphetamine as the treatment. Adapted from Negus and Mello, Drug Alc. Depend. (2003b).
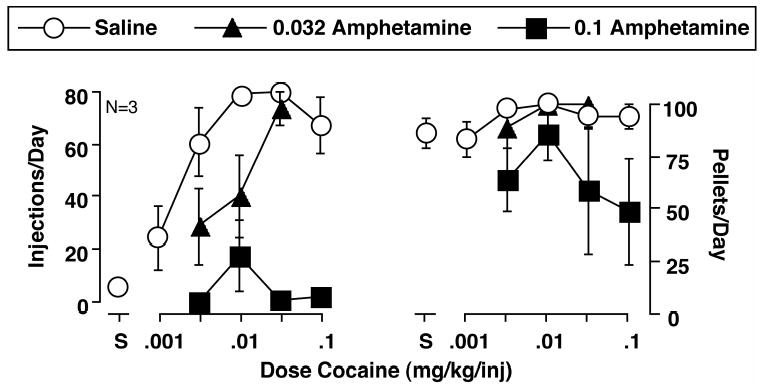
Effects of d-amphetamine on the cocaine self-administration dose-effect curve and concurrent food-maintained responding. Abscissae: Unit dose of cocaine available during daily drug components in mg/kg/injection. Points above S show data collected when saline was the solution available for self-administration. Ordinate (left panel): Mean number of cocaine injections delivered per day during the last three days of each treatment. Ordinate (right panel): Mean number of food pellets (1g) delivered per day during the last three days of each treatment. All points show mean data from three monkeys, and error bars show the SEM. Statistical analysis indicated significant effects on cocaine self-administration of cocaine dose [F(2,4)=10.31; p=0.026] and d-amphetamine dose [F(2,4)=139.8; p=0.0002], but not a significant interaction between cocaine dose and d-amphetamine dose [F(2,8)=1.21; p=0.38]. Both 0.032 and 0.1 mg/kg/hr d-amphetamine produced effects significantly different from saline treatment (p<0.01; Duncan post hoc test). In contrast, there was not a significant effect on food-maintained responding of cocaine dose [F(2,4)=5.37; p=0.074] or d-amphetamine dose [F(2,4)=2.21; p=0.23], and there was not a significant interaction between cocaine dose and d-amphetamine dose [F(2,8)=0.94; p=0.49]. Adapted from Negus and Mello, Drug Alc. Depend. (2003b).
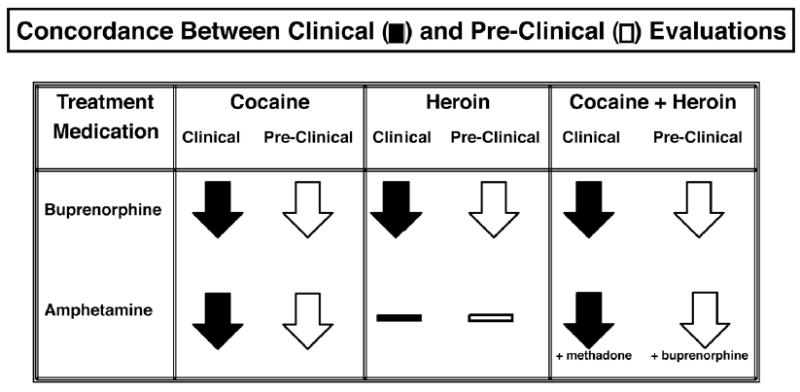
Concordance between clinical and preclinical evaluations of the effects of buprenorphine and of amphetamine on self-administration of cocaine, heroin and cocaine + heroin speedballs. The treatment medication is shown in the far left column. The effects of each treatment medication on cocaine (second column), heroin (third column) and cocaine + heroin speedballs (fourth column) are shown as downward pointing arrows (indicating decreases in drug self-administration) or as horizontal bars (indicating not studied). Clinical studies are shown as black arrows and preclinical studies are shown as white arrows. In row two, column four, amphetamine was studied with methadone or with buprenorphine.
Similar articles
-
Preclinical evaluation of pharmacotherapies for treatment of cocaine and opioid abuse using drug self-administration procedures.Neuropsychopharmacology. 1996 Jun;14(6):375-424. doi: 10.1016/0893-133X(95)00274-H. Neuropsychopharmacology. 1996. PMID: 8726752 Review.
-
Use of Preclinical Drug vs. Food Choice Procedures to Evaluate Candidate Medications for Cocaine Addiction.Curr Treat Options Psychiatry. 2015 Jun;2(2):136-150. doi: 10.1007/s40501-015-0042-9. Curr Treat Options Psychiatry. 2015. PMID: 26009706 Free PMC article.
-
Evaluation of the "Pipeline" for Development of Medications for Cocaine Use Disorder: A Review of Translational Preclinical, Human Laboratory, and Clinical Trial Research.Pharmacol Rev. 2016 Jul;68(3):533-62. doi: 10.1124/pr.115.011668. Pharmacol Rev. 2016. PMID: 27255266 Free PMC article. Review.
-
Utility of preclinical drug versus food choice procedures to evaluate candidate medications for methamphetamine use disorder.Ann N Y Acad Sci. 2017 Apr;1394(1):92-105. doi: 10.1111/nyas.13276. Epub 2016 Dec 9. Ann N Y Acad Sci. 2017. PMID: 27936284 Free PMC article. Review.
-
Drug abuse potential evaluation in animals.Br J Addict. 1991 Dec;86(12):1549-58. doi: 10.1111/j.1360-0443.1991.tb01747.x. Br J Addict. 1991. PMID: 1786486 Review.
Cited by
-
Effects of chronic buspirone treatment on cocaine self-administration.Neuropsychopharmacology. 2013 Feb;38(3):455-67. doi: 10.1038/npp.2012.202. Epub 2012 Oct 17. Neuropsychopharmacology. 2013. PMID: 23072835 Free PMC article.
-
Effects of lorcaserin (Belviq®) on nicotine- and food-maintained responding in non-human primates.Drug Alcohol Depend. 2017 Dec 1;181:94-101. doi: 10.1016/j.drugalcdep.2017.09.008. Epub 2017 Oct 10. Drug Alcohol Depend. 2017. PMID: 29040827 Free PMC article.
-
Effects of chronic varenicline treatment on nicotine, cocaine, and concurrent nicotine+cocaine self-administration.Neuropsychopharmacology. 2014 Apr;39(5):1222-31. doi: 10.1038/npp.2013.325. Epub 2013 Nov 22. Neuropsychopharmacology. 2014. PMID: 24304823 Free PMC article.
-
Mechanisms of withdrawal-associated increases in heroin self-administration: pharmacologic modulation of heroin vs food choice in heroin-dependent rhesus monkeys.Neuropsychopharmacology. 2009 Mar;34(4):899-911. doi: 10.1038/npp.2008.127. Epub 2008 Aug 13. Neuropsychopharmacology. 2009. PMID: 18704098 Free PMC article.
-
Effects of chronic buspirone treatment on nicotine and concurrent nicotine+cocaine self-administration.Neuropsychopharmacology. 2013 Jun;38(7):1264-75. doi: 10.1038/npp.2013.25. Epub 2013 Jan 21. Neuropsychopharmacology. 2013. PMID: 23337868 Free PMC article.
References
References for the Preface
-
- Evans SM, Haney M, Fischman MW, Foltin RW. Limited sex differences in response to “binge” smoked cocaine use in humans. Neuropsychopharmacology. 1999;21:445–454. - PubMed
-
- Fischman MW. The behavioral pharmacology of cocaiine in humans. NIDA Res Monogr. 1984;50:72–91. - PubMed
-
- Fischman, M. W. Cocaine and the amphetamines, in Psychopharmacology, The Third Generation of Progress (Meltzer, H. Y.; ed) New York: Raven Press, 1987, pp. 1543–1553.
-
- Fischman MW. Human drug taking under controlled laboratory conditions. NIDA Res Monogr. 1988;84:196–211. - PubMed
-
- Fischman MW, Foltin RW. A laboratory model for evaluating potential treatment medications in humans. NIDA Res Monogr. 1992;119:165–169. - PubMed
References
-
- Banks CD. Overdose of buprenorphine: Case report. NZ Med J. 1979;89:255–256. - PubMed
-
- Brady, J. V., and Griffiths, R. R. Drug-maintained performance procedures and the assessment of drug-abuse liability, in Predictiing Dependence Liability of Stimulant and Depressant Drugs (Thompson, T.; and Unna, K. R.; eds), Baltimore, MD: University Park Press, 1977, pp. 165–184.
-
- Condelli WS, Fairbank JA, Dennis ML, Rachal JV. Cocaine use by clients in methadone programs: Significance, scope, and behavioral interventions. J Subst Abuse Treat. 1991;8:203–212. - PubMed
-
- Cowan, A., and Lewis, J. W. eds Buprenorphine: Combatting Drug Abuse with a Unique Opioid New York: Wiley-Liss, Inc., 1995.
-
- Deneau G, Yanagita T, Seevers MH. Self-administration of psychoactive substances by the monkey. Psychopharmacologia. 1969;16:30–48. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources