

Transarterial balloon-assisted n-butyl-2-cyanoacrylate embolization of direct carotid cavernous fistulas
- PMID: 16908575
- PMCID: PMC7977514
Transarterial balloon-assisted n-butyl-2-cyanoacrylate embolization of direct carotid cavernous fistulas
Abstract
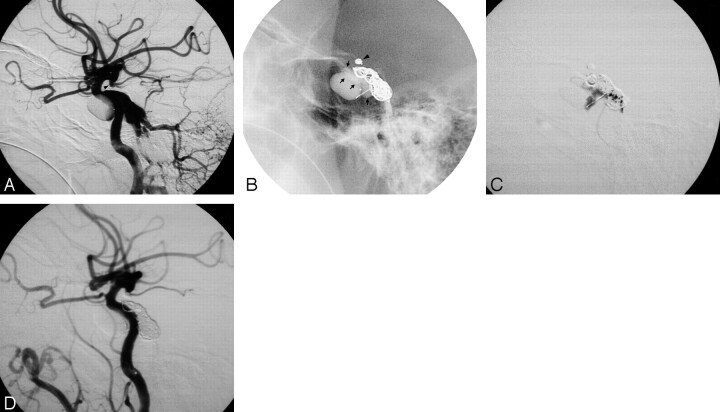
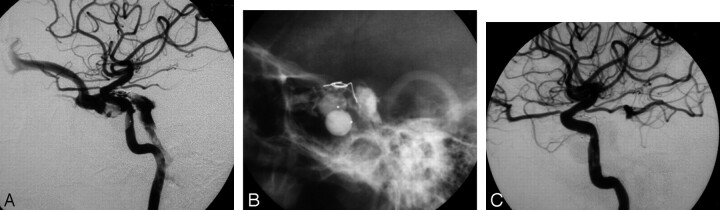
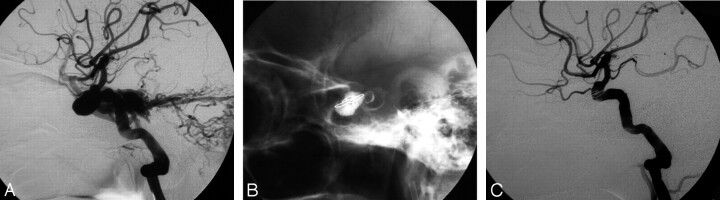
Background and purpose: Transarterial detachable balloon embolization of direct carotid cavernous fistulas (DCCFs) has become an optimal treatment. In a few cases, the parent artery has to be sacrificed to achieve morphologic cure. We present our experience with transarterial balloon-assisted n-butyl-2-cyanoacrylate (n-BCA) embolization of DCCFs in which there was failure to achieve angiographic cure and preservation of parent arteries.
Methods: Of 141 patients with traumatic DCCFs who had been treated by transarterial embolization with occlusion of the fistula and parent artery preservation, 18 received transarterial balloon-assisted n-BCA embolization-6 for residual fistula after the balloons detached, 7 for recurrent fistula because of premature balloon deflation or migration, and 5 for repeated puncture of the detachable balloon by the bony fragment at the cavernous sinus. A total of 27 procedures were performed with an average 1.5 attempts per patient, and the volume of the n-BCA mixture varied from 0.5 to 2.3 mL with a mean of 0.83 mL.
Results: All DCCFs were successfully occluded by the n-BCA mixture with preservation of parent arteries. One patient with a giant cavernous sinus varix had a fatal subarachnoid hemorrhage. One had a recurrence and was treated by internal carotid artery (ICA) occlusion. Five had asymptomatic pseudoaneurysms at the parent artery. There was no adhesion of the n-BCA mixture to the protective balloon or the microcatheter or n-BCA reflux into the parent arteries.
Conclusion: Transarterial balloon-assisted n-BCA embolization is a feasible, efficient, and safe treatment for DCCFs when angiographic cure and ICA preservation are not achieved by transarterial detachable balloon embolization.
Figures

References
-
- Debrun GM, Vinuela F, Fox AJ, et al. Indications for treatment and classification of 132 carotid-cavernous fistulas. Neurosurgery 1988;22:285–89 - PubMed
-
- Goto K, Hieshima GB, Higashida RT, et al. Treatment of direct carotid cavernous sinus fistulae: various therapeutic approaches and results in 148 cases. Acta Radiol Suppl 1986;369:576–79 - PubMed
-
- Kahara VJ, Seppanen S, Kuurne T, et al. Endovascular treatment of carotid-cavernous fistulae. Acta Neurol Scand 1998;98:254–58 - PubMed
-
- Lewis AI, Tomsick TA, Tew JM. Management of 100 consecutive direct carotid-cavernous fistulas: result of treatment with detachable balloons. Neurosurgery 1995;36:239–45 - PubMed
-
- Luo CB, Teng MMH, Yen DH, et al. Endovascular embolization of recurrent traumatic carotid-cavernous fistulas managed previously with detachable balloons. J Trauma 2004;56:1214–20 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous