

Effects of nurse management on the quality of heart failure care in minority communities: a randomized trial
- PMID: 16908918
- PMCID: PMC4307780
- DOI: 10.7326/0003-4819-145-4-200608150-00007
Effects of nurse management on the quality of heart failure care in minority communities: a randomized trial
Abstract
Background: Despite therapies proven effective for heart failure with systolic dysfunction, the condition continues to cause substantial hospitalization, disability, and death, especially among African- American and other nonwhite populations.
Objective: To compare the effects of a nurse-led intervention focused on specific management problems versus usual care among ethnically diverse patients with systolic dysfunction in ambulatory care practices.
Design: Randomized effectiveness trial conducted from September 2000 to September 2002.
Setting: The 4 hospitals in Harlem, New York.
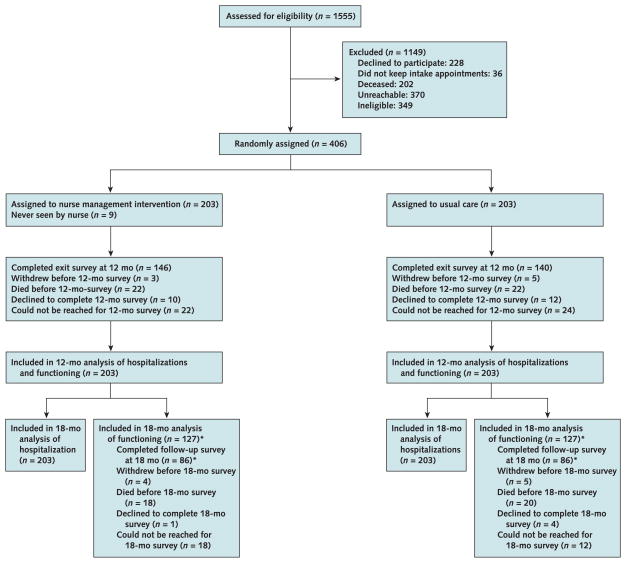
Patients: 406 adults (45.8% were non-Hispanic black adults, 32.5% were Hispanic adults, 46.3% were women, and 36.7% were > or =65 years of age) who met eligibility criteria: systolic dysfunction, English- or Spanish-language speakers, community-dwelling patients, and ambulatory care practice patients.
Intervention: During a 12-month intervention, bilingual nurses counseled patients on diet, medication adherence, and self-management of symptoms through an initial visit and regularly scheduled follow-up telephone calls and facilitated evidence-based changes to medications in discussions with patients' clinicians.
Measurements: Hospitalizations (in 406 of 406 patients during follow-up) and self-reported functioning (in 286 of 406 patients during follow-up) at 12 months.
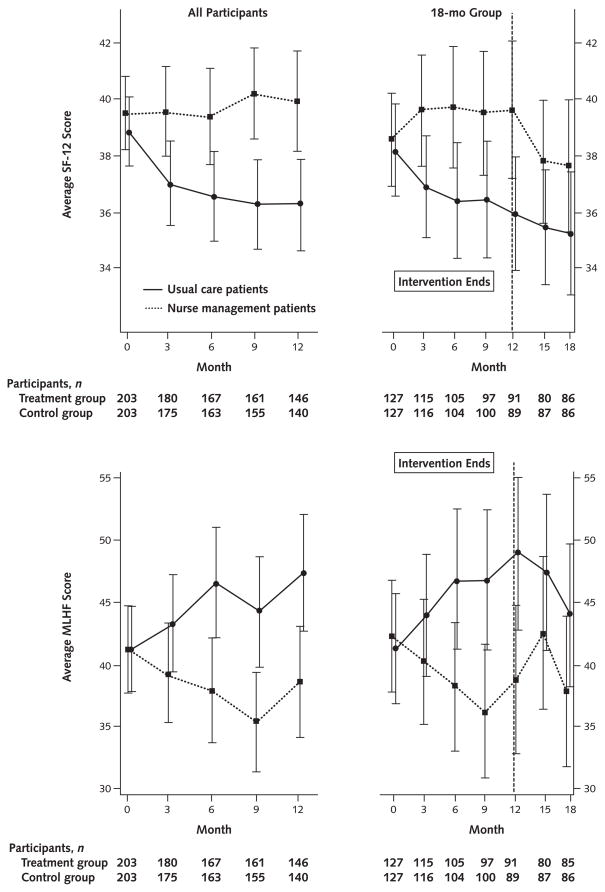
Results: At 12 months, nurse management patients had had fewer hospitalizations (143 hospitalizations vs. 180 hospitalizations; adjusted difference, -0.13 hospitalization/person-year [95% CI, -0.25 to -0.001 hospitalization/person-year]) than usual care patients. They also had better functioning: The Short Form-12 physical component score was 39.9 versus 36.3, respectively (difference, 3.6 [CI, 1.2 to 6.1]), and the Minnesota Living with Heart Failure Questionnaire score was 38.6 versus 47.3, respectively (difference, -8.8 [CI, -15.3 to -2.2]). Through 12 months, 22 deaths occurred in each group and percentages of patients who were hospitalized at least once were similar in each group (30.5% of nurse management patients vs. 36.5% of control patients; adjusted difference, -7.1 percentage points [CI, -16.9 to 2.6 percentage points]).
Limitations: Three nurses at 4 hospitals delivered interventions in this modest-sized trial, and 75% of the participants were from 1 site. It is not clear which aspects of the complex intervention accounted for the results.
Conclusions: Nurse management can improve functioning and modestly lower hospitalizations in ethnically diverse ambulatory care patients who have heart failure with systolic dysfunction. Sustaining improved functioning may require continuing nurse contact.
Conflict of interest statement
Figures
Comment in
-
Health literacy and heart failure care in minority communities.Ann Intern Med. 2007 Feb 20;146(4):312; author reply 312. doi: 10.7326/0003-4819-146-4-200702200-00014. Ann Intern Med. 2007. PMID: 17310058 No abstract available.
Summary for patients in
-
Summaries for patients. The effect of nurse managers on heart failure complications in a minority community.Ann Intern Med. 2006 Aug 15;145(4):I28. doi: 10.7326/0003-4819-145-4-200608150-00001. Ann Intern Med. 2006. PMID: 16908913 No abstract available.
References
-
- Kozak LJ, Hall MJ, Owings MF. Trends in avoidable hospitalizations, 1980–1998. Health Aff (Millwood) 2001;20:225–32. - PubMed
-
- Heart Disease and Stroke Statistics—2005 Update. Dallas, TX: American Heart Association; 2005.
-
- Konstam MA, Dracup K, Baker DW, Bottorff MB, Brooks NH, Dacey RA, et al. Heart Failure: Evaluation and Care of Patients with Left-Ventricular Systolic Dysfunction. Clinical Practice Guideline no. 11. Rockville, MD: Agency for Health Care Policy and Research; Jun, 1994. AHCPR publication no. 94-0612.
-
- Consensus recommendations for the management of chronic heart failure. On behalf of the membership of the advisory council to improve outcomes nationwide in heart failure. Am J Cardiol. 1999;83:1A–38A. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous