

The devil is in the details: trends in avoidable hospitalization rates by geography in British Columbia, 1990-2000
- PMID: 16914056
- PMCID: PMC1564394
- DOI: 10.1186/1472-6963-6-104
The devil is in the details: trends in avoidable hospitalization rates by geography in British Columbia, 1990-2000
Abstract
Background: Researchers and policy makers have focussed on the development of indicators to help monitor the success of regionalization, primary care reform and other health sector restructuring initiatives. Certain indicators are useful in examining issues of equity in service provision, especially among older populations, regardless of where they live. AHRs are used as an indicator of primary care system efficiency and thus reveal information about access to general practitioners. The purpose of this paper is to examine trends in avoidable hospitalization rates (AHRs) during a period of time characterized by several waves of health sector restructuring and regionalization in British Columbia. AHRs are examined in relation to non-avoidable and total hospitalization rates as well as by urban and rural geography across the province.
Methods: Analyses draw on linked administrative health data from the province of British Columbia for 1990 through 2000 for the population aged 50 and over. Joinpoint regression analyses and t-tests are used to detect and describe trends in the data.
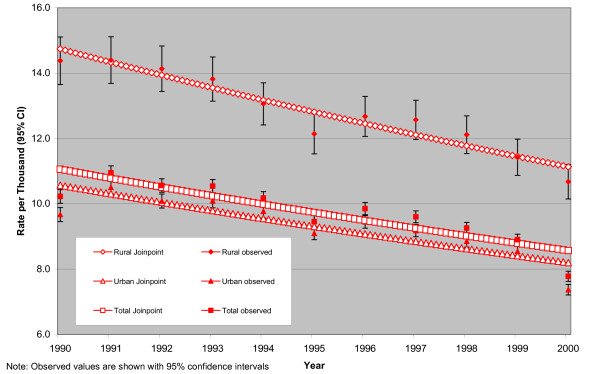
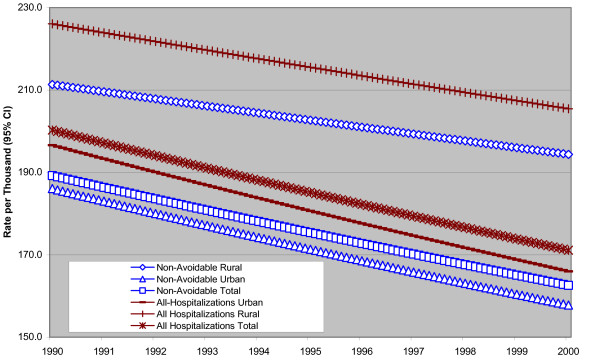
Results: Generally speaking, non-avoidable hospitalizations constitute the vast majority of hospitalizations in a given year (i.e. around 95%) with AHRs constituting the remaining 5% of hospitalizations. Comparing rural areas and urban areas reveals that standardized rates of avoidable, non-avoidable and total hospitalizations are consistently higher in rural areas. Joinpoint regression results show significantly decreasing trends overall; lines are parallel in the case of avoidable hospitalizations, and lines are diverging for non-avoidable and total hospitalizations, with the gap between rural and urban areas being wider at the end of the time interval than at the beginning.
Conclusion: These data suggest that access to effective primary care in rural communities remains problematic in BC given that rural areas did not make any gains in AHRs relative to urban areas under recent health sector restructuring initiatives. It remains important to continue to monitor the discrepancy between them as a reflection of inequity in service provision. In addition, it is important to consider alternative explanations for the observed trends paying particular attention to the needs of rural and urban populations and the factors influencing local service provision.
Figures
Similar articles
-
A model for identifying and ranking need for trauma service in nonmetropolitan regions based on injury risk and access to services.J Trauma. 2008 Jul;65(1):54-62. doi: 10.1097/TA.0b013e31815efe0e. J Trauma. 2008. PMID: 18580511
-
A protocol for determining differences in consistency and depth of palliative care service provision across community sites.Health Soc Care Community. 2010 Sep;18(5):537-48. doi: 10.1111/j.1365-2524.2010.00933.x. Epub 2010 Jun 16. Health Soc Care Community. 2010. PMID: 20561070
-
Transfers to acute care hospitals at the end of life: do rural/remote regions differ from urban regions?Rural Remote Health. 2010 Jan-Mar;10(1):1281. Epub 2010 Jan 12. Rural Remote Health. 2010. PMID: 20095758
-
Helping policy-makers address rural health access problems.Aust J Rural Health. 2013 Apr;21(2):61-71. doi: 10.1111/ajr.12023. Aust J Rural Health. 2013. PMID: 23586567 Review.
-
[Avoidable hospitalizations: the sole responsibility of primary care?].Rev Epidemiol Sante Publique. 2014 Aug;62(4):225-36. doi: 10.1016/j.respe.2014.04.005. Epub 2014 Jul 11. Rev Epidemiol Sante Publique. 2014. PMID: 25026885 Review. French.
Cited by
-
Geographic variation in preventable hospitalisations across Canada: a cross-sectional study.BMJ Open. 2020 May 15;10(5):e037195. doi: 10.1136/bmjopen-2020-037195. BMJ Open. 2020. PMID: 32414831 Free PMC article.
-
Comparison of two methods to report potentially avoidable hospitalizations in France in 2012: a cross-sectional study.BMC Health Serv Res. 2015 Jan 22;15:4. doi: 10.1186/s12913-014-0661-7. BMC Health Serv Res. 2015. PMID: 25608760 Free PMC article.
-
The rural tax: comprehensive out-of-pocket costs associated with patient travel in British Columbia.BMC Health Serv Res. 2021 Aug 21;21(1):854. doi: 10.1186/s12913-021-06833-2. BMC Health Serv Res. 2021. PMID: 34419025 Free PMC article.
-
Exploration of Preventable Hospitalizations for Colorectal Cancer with the National Cancer Control Program in Taiwan.Int J Environ Res Public Health. 2021 Sep 3;18(17):9327. doi: 10.3390/ijerph18179327. Int J Environ Res Public Health. 2021. PMID: 34501914 Free PMC article.
-
Investigation of rural-urban differences in hospitalization for ambulatory care-sensitive conditions: Analysis of linked survey, hospitalization, and tax data from Canada.J Rural Health. 2025 Jan;41(1):e70010. doi: 10.1111/jrh.70010. J Rural Health. 2025. PMID: 40029101 Free PMC article.
References
-
- Health Canada . Certain Circumstances: Issues in Equity and Responsiveness in Access to Health Care in Canada. Ottawa: Health Canada; 2001. Access to health services for underserved populations in Canada; pp. 1–60.
-
- Millman M, ed . Access to Health Care in America: Report of the Committee on Monitoring Access to Personal Health Care Services. Institute of Medicine, Washington, D.C., National Academy Press; 1993.
-
- Joseph AE, Phillips DR. Accessibility & Utilization: Geographical Perspectives on Health Care Delivery. London: Harper & Row; 1984.
-
- Lin G, Allan DE, Penning MJ. Examining distance effects on hospitalizations using GIS: a study of three health regions in British Columbia, Canada. Environment and Planning A. 2002;34:2037–2053. doi: 10.1068/a3528. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
