

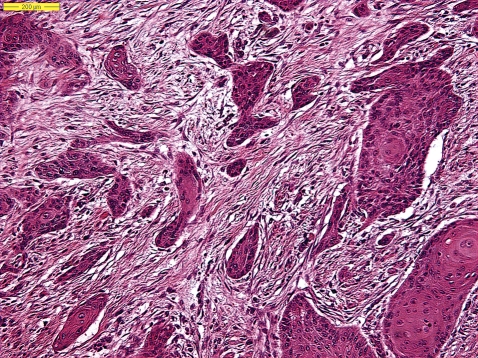
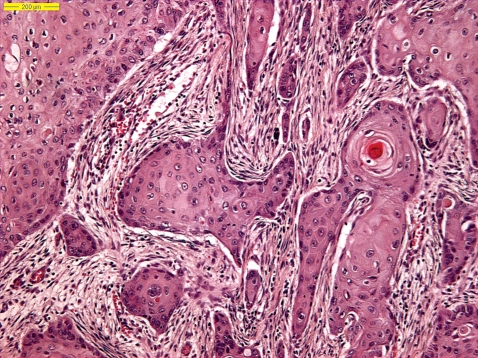
Histopathological characteristics of metastasizing squamous cell carcinoma of the skin and lips
- PMID: 16918972
- PMCID: PMC1619204
- DOI: 10.1111/j.1365-2559.2006.02472.x
Histopathological characteristics of metastasizing squamous cell carcinoma of the skin and lips
Abstract
Aims: The reported incidence of metastasis from squamous cell carcinoma (SCC) of the skin and lip varies between 0.5% and 16%. Clinical and histopathological criteria have been proposed to identify tumours that may have an increased risk of metastasis. The aim of this study was to define such high-risk tumours, especially since the incidence of SCC of the skin is increasing.
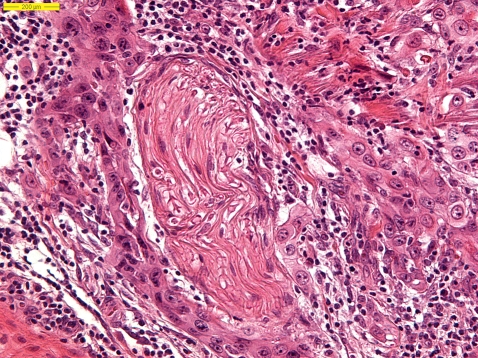
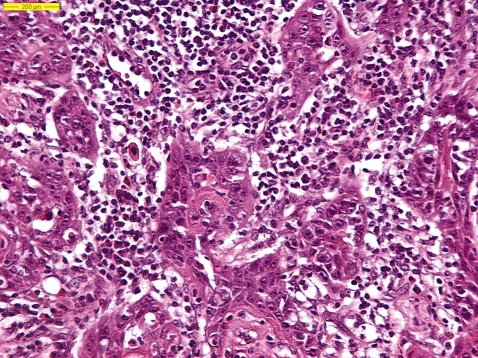
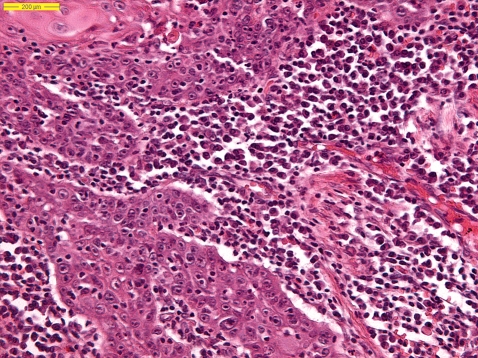
Methods and results: Histopathological features of metastasized skin and lip tumours and a matched group of non-metastasizing tumours were reassessed. Characteristics studied were: tumour width, excision margins, histological subtype, Clark level, Breslow depth, tumour differentiation, inflammation, perineural and angio-invasive growth, ulceration and desmoplasia. Data were statistically analysed separately for skin and labial lesions. Desmoplasia, Clark level, Breslow depth, maximum diameter, angio-invasion, grading, perineural invasion, plasma cells and eosinophilic inflammatory response proved to be statistically significantly related to metastasis of skin tumours. Breslow depth, plasma cells and grading appeared to be statistically significantly related to metastasis of SCC of the lips.
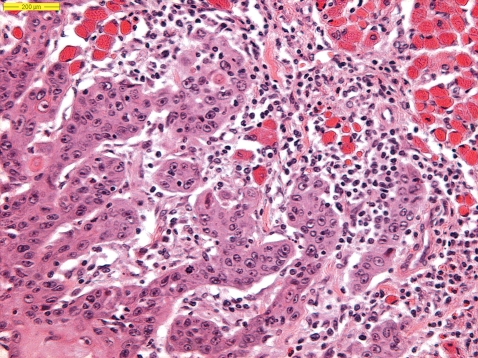
Conclusions: A typical metastatic SCC showed: a tumour width of at least 15 mm, a vertical tumour thickness (=Breslow) of at least 2 mm, less differentiation, presence of desmoplasia and an inflammatory response with eosinophils and plasma cells.
Figures
Similar articles
-
Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: a prospective study.Lancet Oncol. 2008 Aug;9(8):713-20. doi: 10.1016/S1470-2045(08)70178-5. Epub 2008 Jul 9. Lancet Oncol. 2008. PMID: 18617440
-
[Desmoplastic squamous epithelial carcinoma of the skin and lower lip. A morphologic entity with great risk of metastasis and recurrence].Hautarzt. 1998 Feb;49(2):104-8. doi: 10.1007/s001050050708. Hautarzt. 1998. PMID: 9551331 German.
-
Desmoplastic squamous cell carcinoma of skin and vermilion surface: a highly malignant subtype of skin cancer.Cancer. 1997 Mar 1;79(5):915-9. doi: 10.1002/(sici)1097-0142(19970301)79:5<915::aid-cncr7>3.0.co;2-a. Cancer. 1997. PMID: 9041153
-
Squamocellular Carcinoma of the Skin: Clinicopathological Features Predicting the Involvement of the Surgical Margins and Review of the Literature.Dermatology. 2016;232(3):279-84. doi: 10.1159/000444051. Epub 2016 Mar 31. Dermatology. 2016. PMID: 27028227 Review.
-
Prognostic factors for local recurrence, metastasis, and survival rates in squamous cell carcinoma of the skin, ear, and lip. Implications for treatment modality selection.J Am Acad Dermatol. 1992 Jun;26(6):976-90. doi: 10.1016/0190-9622(92)70144-5. J Am Acad Dermatol. 1992. PMID: 1607418 Review.
Cited by
-
Eosinophils and oral squamous cell carcinoma: a short review.J Oncol. 2009;2009:310132. doi: 10.1155/2009/310132. Epub 2009 Dec 16. J Oncol. 2009. PMID: 20049171 Free PMC article.
-
Quantitative Evaluation of Tumour--Associated Tissue Eosinophilia and Cyclo-oxegenase-2 Gene in Oral Cancer Patients with Assessment of Long Term Outcomes.Pathol Oncol Res. 2016 Apr;22(2):385-92. doi: 10.1007/s12253-015-0016-7. Epub 2015 Nov 17. Pathol Oncol Res. 2016. PMID: 26577687
-
Management of Cutaneous Squamous Cell Carcinoma of the Scalp: The Role of Imaging and Therapeutic Approaches.Cancers (Basel). 2024 Feb 4;16(3):664. doi: 10.3390/cancers16030664. Cancers (Basel). 2024. PMID: 38339415 Free PMC article. Review.
-
CYFIP1 is directly controlled by NOTCH1 and down-regulated in cutaneous squamous cell carcinoma.PLoS One. 2017 Apr 14;12(4):e0173000. doi: 10.1371/journal.pone.0173000. eCollection 2017. PLoS One. 2017. PMID: 28410392 Free PMC article.
-
Molecular markers in cutaneous squamous cell carcinoma.Int J Surg Oncol. 2011;2011:231475. doi: 10.1155/2011/231475. Epub 2011 Aug 9. Int J Surg Oncol. 2011. PMID: 22312497 Free PMC article.
References
-
- Alam M, Ratner D. Cutaneous squamous cell carcinoma. N Engl. J. Med. 2001;344:975–983. - PubMed
-
- Marks R. Squamous cell carcinoma. Lancet. 1996;347:735–738. - PubMed
-
- Kwa RE, Campagna K, Moy RL. Biology of cutaneous squamous cell carcinoma. J. Am. Acad. Dermatol. 1992;26:1–26. - PubMed
-
- Maguire B, Smith NP. Histopathology of cutaneous squamous cell carcinoma. Clin. Dermatol. 1995;13:559–568. - PubMed
-
- Czarnecki D, Staples M, Mar A, et al. Metastases from squamous cell carcinoma of the skin in Southern Australia. Dermatology. 1994;189:52–54. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
