

Stereotactic, single-dose irradiation of stage I non-small cell lung cancer and lung metastases
- PMID: 16919172
- PMCID: PMC1579222
- DOI: 10.1186/1748-717X-1-30
Stereotactic, single-dose irradiation of stage I non-small cell lung cancer and lung metastases
Abstract
Background: We prospectively reviewed response rates, local control, and side effects after non-fractionated stereotactic high single-dose body radiation therapy for lung tumors.
Methods: Fifty-eight patients underwent radiosurgery involving single-dose irradiation. With 25 patients, 31 metastases in the lungs were irradiated; with each of 33 patients, stage I non-small cell lung cancer (NSCLC) was subject to irradiation. The standard dose prescribed to the isocenter was 30 Gy with an axial safety margin of 10 mm and a longitudinal safety margin of 15 mm. The planning target volume (PTV) was defined using three CT scans with reference to the phases of respiration so that the movement span of the clinical target volume (CTV) was enclosed.
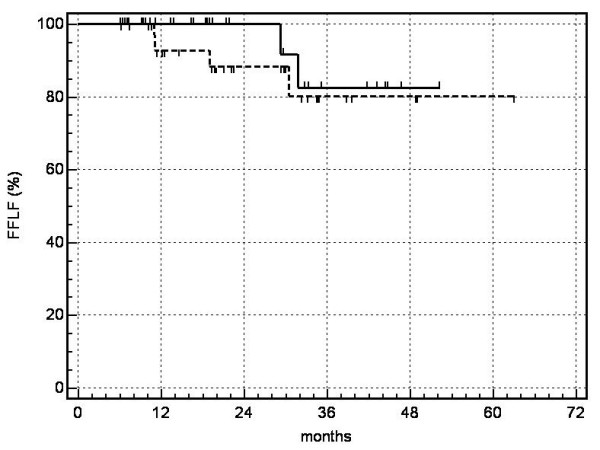
Results: The volume of the metastases (CTV) varied from 2.8 to 55.8 cm3 (median: 6.0 cm3) and the PTV varied from 12.2 to 184.0 cm3 (median: 45.0 cm3). The metastases ranged from 0.7 to 4.5 cm in largest diameter. The volume of the bronchial carcinomas varied from 4.2 to 125.4 cm3 (median: 17.5 cm3) and the PTV from 15.6 to 387.3 cm3 (median: 99.8 cm3). The bronchial carcinomas ranged from 1.7 to 10 cm in largest diameter. Follow-up periods varied from 6.8 to 63 months (median: 22 months for metastases and 18 months for NSCLC). Local control was achieved with 94% of NSCLC and 87% of metastases. No serious symptomatic side effects were observed. According to the Kaplan-Meier method the overall survival probability rates of patients with lung metastases were as follows: 1 year: 97%, 2 years: 73%, 3 years: 42%, 4 years: 42%, 5 years: 42% (median survival: 26 months); of those with NSCLC: 1 year: 83%, 2 years: 63%, 3 years: 53%, 4 years: 39%: (median survival: 20.4 months).
Conclusion: Non-fractionated single-dose irradiation of metastases in the lungs or of small, peripheral bronchial carcinomas is an effective and safe form of local treatment and might become a viable alternative to invasive techniques.
Figures
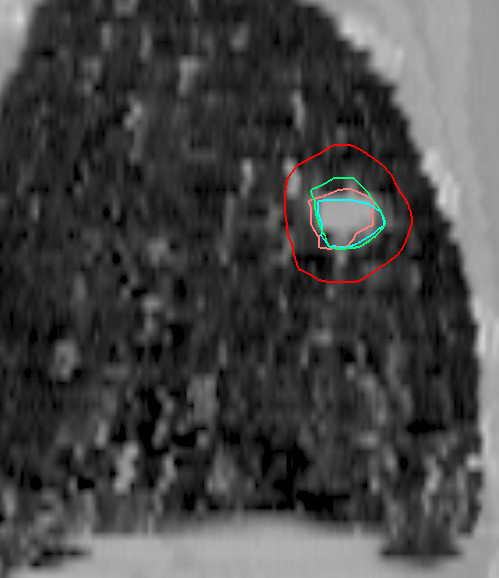
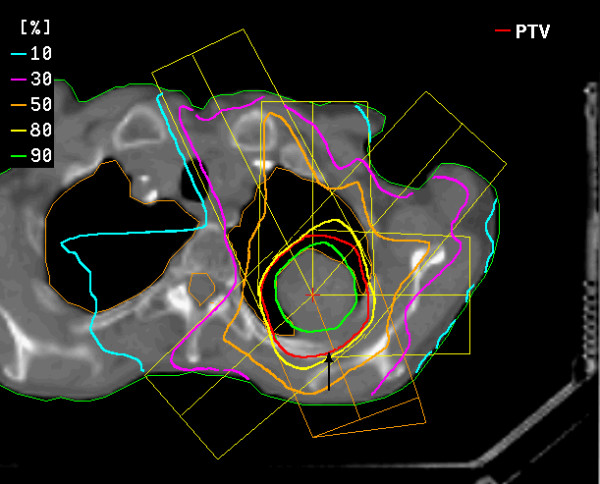
 ) and dose distribution for single-dose irradiation of a bronchial carcinoma using six coplanar portals (course of remission see figures figures 3a, b, c, d).
) and dose distribution for single-dose irradiation of a bronchial carcinoma using six coplanar portals (course of remission see figures figures 3a, b, c, d).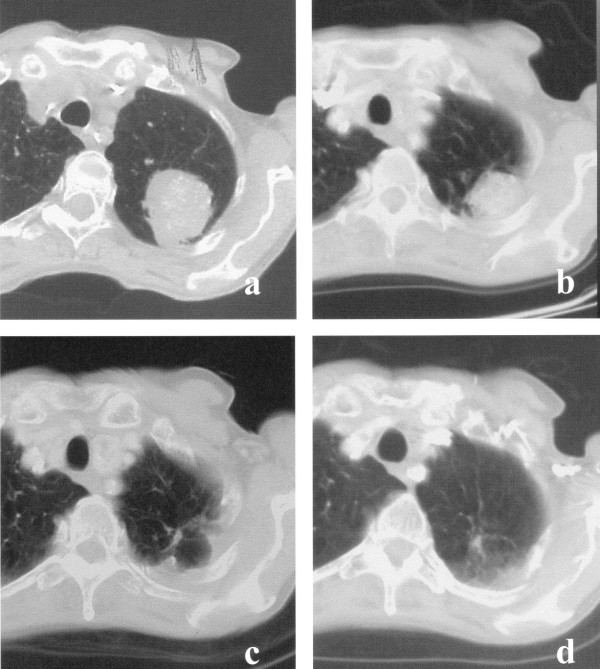
 NSCLC
NSCLC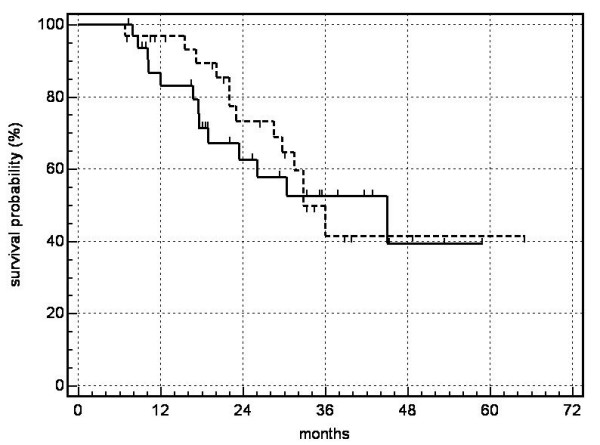 NSCLC.
NSCLC.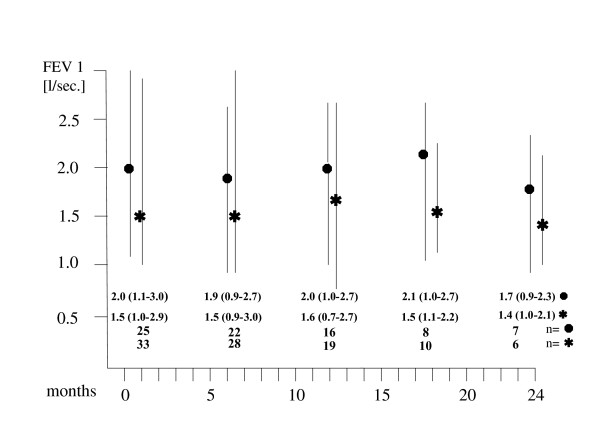
 bronchial carcinomas, median and range values for patients (n) alive and available at the specified follow-up periods).
bronchial carcinomas, median and range values for patients (n) alive and available at the specified follow-up periods).References
-
- Lax I, Blomgren H, Larson D, Näslund I. Extracranial stereotactic radiosurgery of localized targets. J Radiosurgery. 1998;1:135–148. doi: 10.1023/B:JORA.0000010898.87146.2e. - DOI
-
- Blomgren H, Lax I, Näslund I, Svanström R. Stereotactic high dose fraction radiation therapy of extracranial tumors using an accelerator. Clinical experience of the first thirty-one patiens. Acta Oncol. 1995;34:861–870. - PubMed
-
- Vogl TJ, Mack MG, Roggan A, Straub R, Eichler KC, Müller PK, Knappe RV, Felix R. Internally cooled Power laser for MR-guided interstitial laser-induced thermotherapy of liver lesions: Initial clinical results. Radiology. 1998;209:381–385. - PubMed
-
- Vogl TJ, Straub R, Eichler K, Woitaschek D, Mack MG. Malignant liver tumors treated with MR imaging-guided laser-induced thermotherapy. Experience with complications in 899 patients (2,520 lesions) Radiology. 2002;225:367–377. - PubMed
-
- Hosten N, Stier A, Weigel C, Kirsch M, Puls R, Nerger U, Jahn D, Stroszczynski C, Heidecke CD, Speck U. Laser-Induced Thermotherapy (LITT) of Lung Metastases: Description of a Miniaturized Applicator, and Initial Treatment of Patients. Fortschr Röntgenstr. 2003;175:393–400. doi: 10.1055/s-2003-37830. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
