

Cardiovascular disease prevention with a multidrug regimen in the developing world: a cost-effectiveness analysis
- PMID: 16920473
- PMCID: PMC2365896
- DOI: 10.1016/S0140-6736(06)69252-0
Cardiovascular disease prevention with a multidrug regimen in the developing world: a cost-effectiveness analysis
Abstract
Background: Cardiovascular disease is the leading cause of death, with 80% of cases occurring in developing countries. We therefore aimed to establish whether use of evidence-based multidrug regimens for patients at high risk for cardiovascular disease would be cost-effective in low-income and middle-income countries.
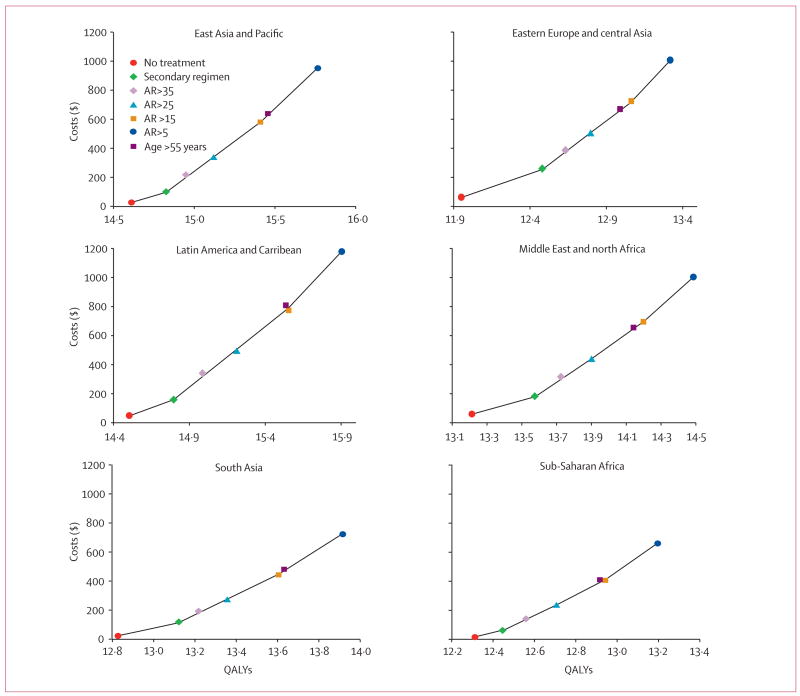
Methods: We used a Markov model to do a cost-effectiveness analysis with two combination regimens. For primary prevention, we used aspirin, a calcium-channel blocker, an angiotensin-converting-enzyme inhibitor, and a statin, and assessed them in four groups with different thresholds of absolute risks for cardiovascular disease. For secondary prevention, we assessed the same combination of drugs in one group, but substituted a beta blocker for the calcium-channel blocker. To compare strategies, we report incremental cost-effectiveness ratios (ICER), in US dollars per quality-adjusted life-year (QALY).
Findings: We recorded that preventive strategies could result in a 2-year gain in life expectancy. Across six developing World Bank regions, primary prevention yielded ICERs of US746-890 dollars/QALY gained for patients with a 10-year absolute risk of cardiovascular disease greater than 25%, and 1039-1221 dollars/QALY gained for those with an absolute risk greater than 5%. ICERs for secondary prevention ranged from 306 dollars/QALY to 388 dollars/QALY gained.
Interpretation: Regimens of aspirin, two blood-pressure drugs, and a statin could halve the risk of death from cardiovascular disease in high-risk patients. This approach is cost-effective according to WHO recommendations, and is robust across several estimates of drug efficacy and of treatment cost. Developing countries should encourage the use of these inexpensive drugs that are currently available for both primary and secondary prevention.
Conflict of interest statement
Conflict of interest statement
We declare that we have no conflict of interest.
Figures
Comment in
-
Prevention of cardiovascular disease with a polypill.Lancet. 2007 Jan 20;369(9557):185-6; author reply 186. doi: 10.1016/S0140-6736(07)60097-X. Lancet. 2007. PMID: 17240275 No abstract available.
-
Is a multidrug regimen cost-effective for the prevention of cardiovascular disease in resource-poor countries?Nat Clin Pract Cardiovasc Med. 2007 Mar;4(3):130-2. doi: 10.1038/ncpcardio0799. Epub 2007 Jan 30. Nat Clin Pract Cardiovasc Med. 2007. PMID: 17262058 No abstract available.
References
-
- Mathers CD, Lopez A, Stein C, et al. Working paper 18. Bethesda, MD: Disease Control Priorities Project; 2005. Deaths and disease burden by cause: global burden of disease estimates for 2001 by World Bank Country Groups.
-
- Fuster V, Voûte J. MDGs: chronic diseases are not on the agenda. Lancet. 2005;366:1512–14. - PubMed
-
- Horton R. The neglected epidemic of chronic disease. Lancet. 2005;366:1514. - PubMed
-
- World Bank. World development indicators. Washington, DC: World Bank; 2002.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
