

State of the Art. A structural and functional assessment of the lung via multidetector-row computed tomography: phenotyping chronic obstructive pulmonary disease
- PMID: 16921136
- PMCID: PMC2647643
- DOI: 10.1513/pats.200603-086MS
State of the Art. A structural and functional assessment of the lung via multidetector-row computed tomography: phenotyping chronic obstructive pulmonary disease
Abstract
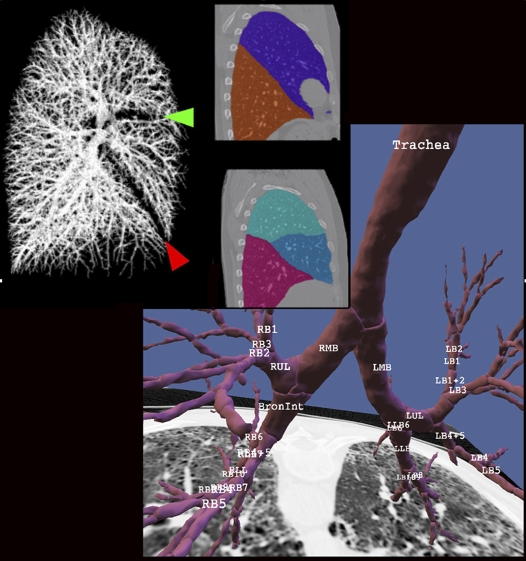
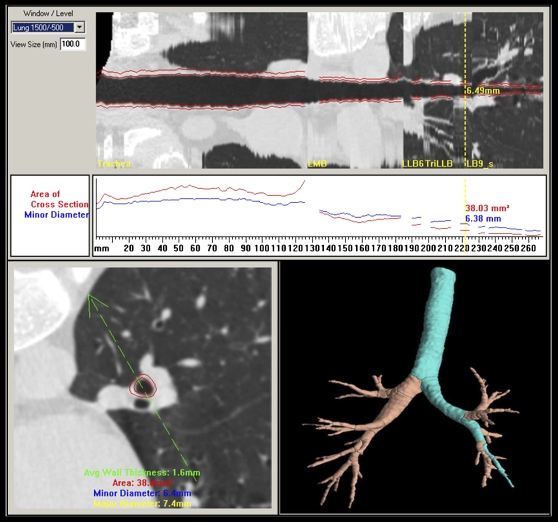
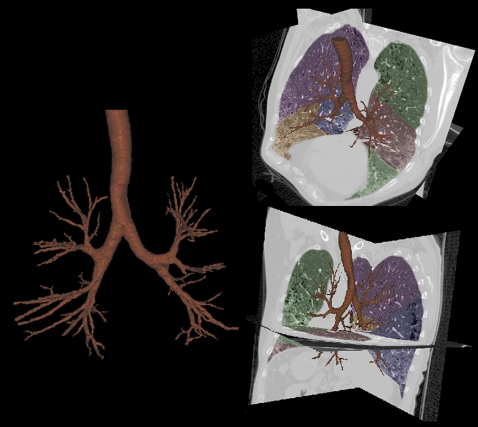
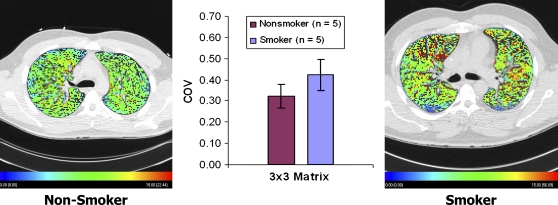
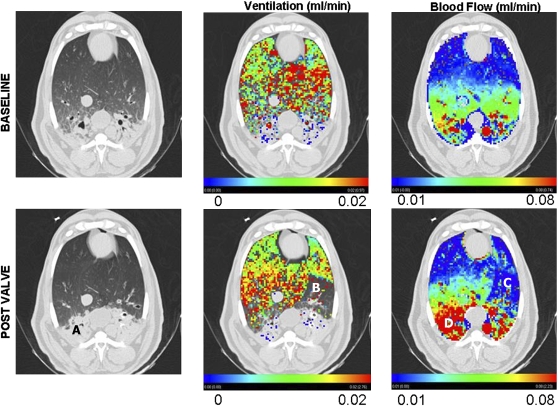
With advances in multidetector-row computed tomography (MDCT), it is now possible to image the lung in 10 s or less and accurately extract the lungs, lobes, and airway tree to the fifth- through seventh-generation bronchi and to regionally characterize lung density, texture, ventilation, and perfusion. These methods are now being used to phenotype the lung in health and disease and to gain insights into the etiology of pathologic processes. This article outlines the application of these methodologies with specific emphasis on chronic obstructive pulmonary disease. We demonstrate the use of our methods for assessing regional ventilation and perfusion and demonstrate early data that show, in a sheep model, a regionally intact hypoxic pulmonary vasoconstrictor (HPV) response with an apparent inhibition of HPV regionally in the presence of inflammation. We present the hypothesis that, in subjects with pulmonary emphysema, one major contributing factor leading to parenchymal destruction is the lack of a regional blunting of HPV when the regional hypoxia is related to regional inflammatory events (bronchiolitis or alveolar flooding). If maintaining adequate blood flow to inflamed lung regions is critical to the nondestructive resolution of inflammatory events, the pathologic condition whereby HPV is sustained in regions of inflammation would likely have its greatest effect in the lung apices where blood flow is already reduced in the upright body posture.
Figures
References
-
- Remy-Jardin M, Edme JL, Boulenguez C, Remy J, Mastora I, Sobaszek A. Longitudinal follow-up study of smoker's lung with thin-section CT in correlation with pulmonary function tests. Radiology 2002;222:261–270. - PubMed
-
- Moonen M, Xu J, Johansson A, Thylen A, Bake B. Effects of lung volume reduction surgery on distribution of ventilation and perfusion. Clin Physiol Funct Imaging 2005;25:152–157. - PubMed
-
- Xu JH, Moonen M, Johansson A, Bake B. Distribution of ventilation-to-perfusion ratios analysed in planar scintigrams of emphysematous patients. Clin Physiol 2000;20:89–94. - PubMed
-
- Cederlund K, Hogberg S, Jorfeldt L, Larsen F, Norman M, Rasmussen E, Tylen U. Lung perfusion scintigraphy prior to lung volume reduction surgery. Acta Radiol 2003;44:246–251. - PubMed
-
- Hunsaker AR, Ingenito EP, Reilly JJ, Costello P. Lung volume reduction surgery for emphysema: correlation of CT and V̇/Q̇ imaging with physiologic mechanisms of improvement in lung function. Radiology 2002;222:491–498. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical