

Open versus laparoscopic pyloromyotomy for pyloric stenosis: a prospective, randomized trial
- PMID: 16926562
- PMCID: PMC1856534
- DOI: 10.1097/01.sla.0000234647.03466.27
Open versus laparoscopic pyloromyotomy for pyloric stenosis: a prospective, randomized trial
Abstract
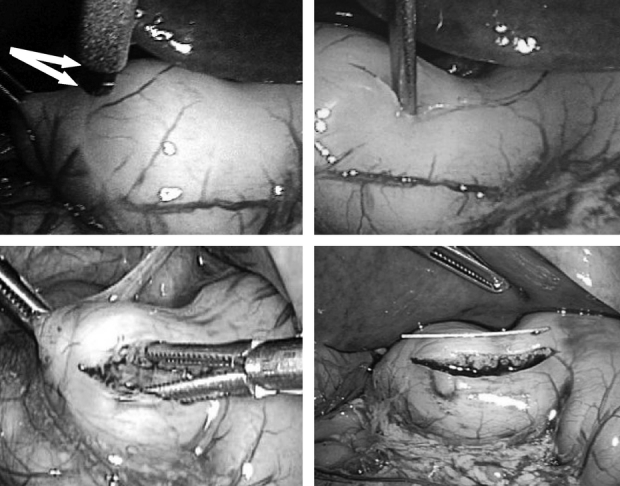
Background: Pyloric stenosis, the most common surgical condition of infants, is treated by longitudinal myotomy of the pylorus. Comparative studies to date between open and laparoscopic pyloromyotomy have been retrospective and report conflicting results. To scientifically compare the 2 techniques, we conducted the first large prospective, randomized trial between the 2 approaches.
Methods: After obtaining IRB approval, subjects with ultrasound-proven pyloric stenosis were randomized to either open or laparoscopic pyloromyotomy. Postoperative pain management, feeding schedule, and discharge criteria were identical for both groups. Operating time, postoperative emesis, analgesia requirements, time to full feeding, length of hospitalization after operation, and complications were compared.
Results: From April 2003 through March 2006, 200 patients were enrolled in the study. There were no significant differences in operating time, time to full feeding, or length of stay. There were significantly fewer number of emesis episodes and doses of analgesia given in the laparoscopic group. One mucosal perforation and one incisional hernia occurred in the open group. Late in the study, 1 patient in the laparoscopic group was converted to the open operation. A wound infection occurred in 4 of the open patients compared with 2 of the laparoscopic patients (P = 0.68).
Conclusions: There is no difference in operating time or length of recovery between open and laparoscopic pyloromyotomy. However, the laparoscopic approach results in less postoperative pain and reduced postoperative emesis. In addition, there was a fewer number of complications in the laparoscopic group. Finally, patients approached laparoscopically will likely display superior cosmetic outcomes with long-term follow-up.
Figures

Comment in
-
Is open or laparoscopic pyloromyotomy better for hypertrophic pyloric stenosis?Nat Clin Pract Gastroenterol Hepatol. 2007 Apr;4(4):196-7. doi: 10.1038/ncpgasthep0764. Epub 2007 Feb 27. Nat Clin Pract Gastroenterol Hepatol. 2007. PMID: 17325722 No abstract available.
References
-
- Alain JL, Grousseau D, Terrier G. Extramucosal pyloromyotomy by laparoscopy. Surg Endosc. 1991;5:174–175. - PubMed
-
- Greason KL, Thompson WR, Downey EC, et al. Laparoscopic pyloromyotomy for infantile hypertrophic pyloric stenosis: report of 11 cases. J Pediatr Surg. 1995;30:1571–1574. - PubMed
-
- Bufo AJ, Merry C, Shah R, et al. Laparoscopic pyloromyotomy: a safer technique. Pediatr Surg Int. 1998;13:240–242. - PubMed
-
- Alain JL, Grousseau D, Longis B, et al. Laparoscopic pyloromyotomy for infantile hypertrophic stenosis. J Pediatr Surg. 1996;31:1197–1198. - PubMed
-
- Hamada Y, Tsui M, Kogata M, et al. Surgical technique of laparoscopic pyloromyotomy for infantile hypertrophic pyloric stenosis. Surg Today. 1995;25:754–756. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
