

Patterns of errors contributing to trauma mortality: lessons learned from 2,594 deaths
- PMID: 16926563
- PMCID: PMC1856538
- DOI: 10.1097/01.sla.0000234655.83517.56
Patterns of errors contributing to trauma mortality: lessons learned from 2,594 deaths
Abstract
Objective: To identify patterns of errors contributing to inpatient trauma deaths.
Methods: All inpatient trauma deaths at a high-volume level I trauma center from 1996 to 2004 inclusive were audited. Data were collected with daily trauma registry chart abstraction, weekly morbidity and mortality reports, hospital quality assurance reports, and annual trauma registry analyses of risk of death using TRISS and HARM methodology. Deaths that met criteria for low to medium probability of mortality or those with quality of care concerns were analyzed for errors and then subjected to 3-stage peer review at weekly departmental, monthly hospital, and annual regional forums. Patterns of errors were constructed from the compiled longitudinal data.
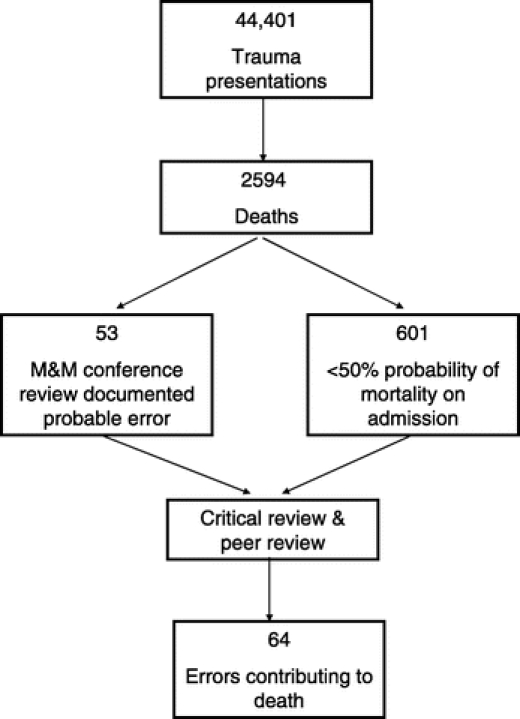
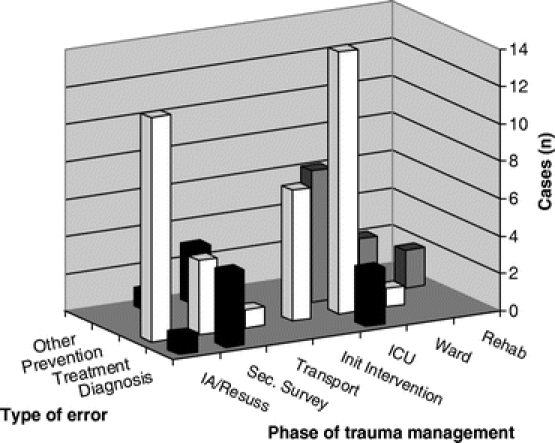
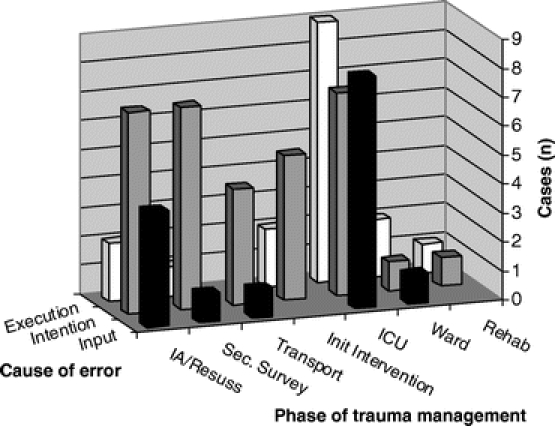
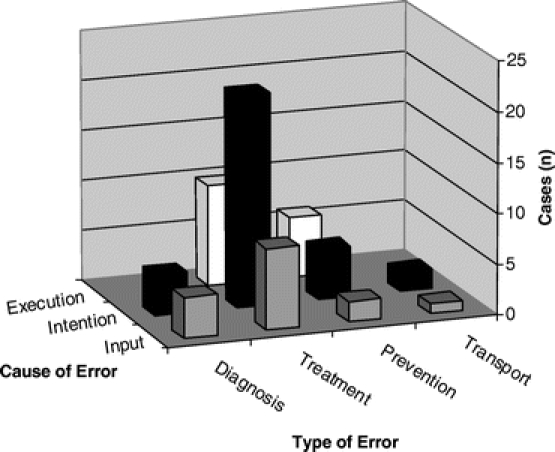
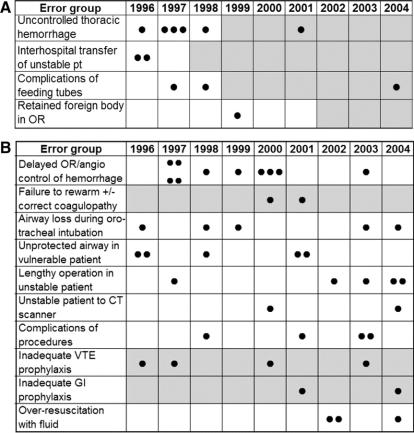
Results: In 9 years, there were 44,401 trauma patient admissions and 2,594 deaths (5.8%), of which 601 met low to medium mortality risks. Sixty-four patients (0.14% admissions, 2.47% deaths) had recognized errors in care that contributed to their death. Important error patterns included: failure to successfully intubate, secure or protect an airway (16%), delayed operative or angiographic control of acute abdominal/pelvic hemorrhage (16%), delayed intervention for ongoing intrathoracic hemorrhage (9%), inadequate DVT or gastrointestinal prophylaxis (9%), lengthy initial operative procedures rather than damage control surgery in unstable patients (8%), over-resuscitation with fluids (5%), and complications of feeding tubes (5%). Resulting data-directed institutional and regional trauma system policy changes have demonstrably reduced the incidence of associated error-related deaths.
Conclusions: Preventable deaths will occur even in mature trauma systems. This review has identified error patterns that are likely common in all trauma systems, and for which policy interventions can be effectively targeted.
Figures
References
-
- Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients: results of the Harvard Medical Practice Study I. N Engl J Med. 1991;324:370–376. - PubMed
-
- Leape LL, Brennan TA, Laird N, et al. The nature of adverse events in hospitalized patients: results of the Harvard Medical Practice Study II. N Engl J Med. 1991;324:377–384. - PubMed
-
- Wilson RM, Runciman WB, Gibberd RW, et al. The quality in Australian Health Care Study. Med J Aust. 1995;163:458–471. - PubMed
-
- Famularo G, Salvini P, Terranova A, et al. Clinical errors in emergency medicine: experience at the emergency department of an Italian Teaching Hospital. Acad Emerg Med. 2000;7:1278–1281. - PubMed
-
- Zollinger R. Traffic injuries: a surgical problem. AMA Arch Surg. 1955;70:694–800. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
