

Surgery increases survival in patients with gastrinoma
- PMID: 16926567
- PMCID: PMC1856542
- DOI: 10.1097/01.sla.0000234802.44320.a5
Surgery increases survival in patients with gastrinoma
Abstract
Objective: To determine whether the routine use of surgical exploration for gastrinoma resection/cure in 160 patients with Zollinger-Ellison syndrome (ZES) altered survival compared with 35 ZES patients who did not undergo surgery.
Summary background data: The role of routine surgical exploration for resection/cure in patients with ZES has been controversial since the original description of this disease in 1955. This controversy continues today, not only because medical therapy for acid hypersecretion is so effective, but also in large part because no studies have shown an effect of tumor resection on survival.
Methods: Long-term follow-up of 160 ZES patients who underwent routine surgery for gastrinoma/resection/cure was compared with 35 patients who had similar disease but did not undergo surgery for a variety of reasons. All patients had preoperative CT, MRI, ultrasound; if unclear, angiography and somatostatin receptor scintigraphy since 1994 to determine resectability. At surgery, all had the same standard ZES operation. All patients were evaluated yearly with imaging studies and disease activity studies.
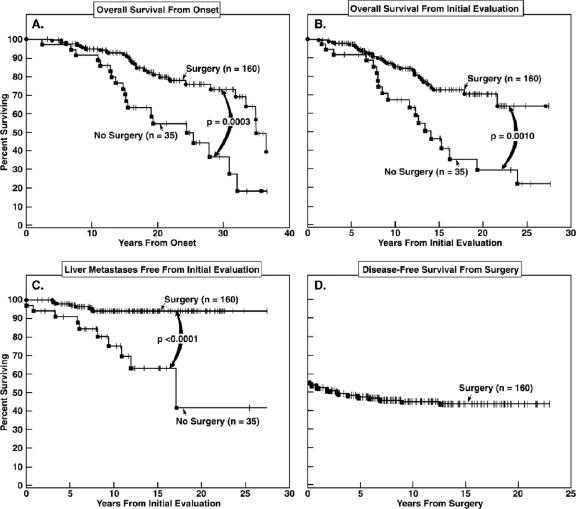
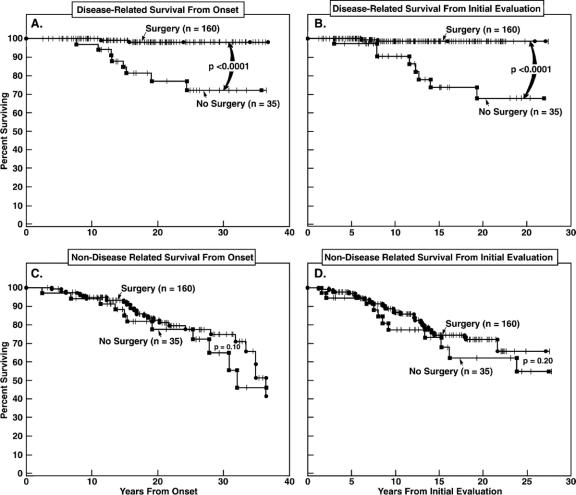
Results: The 35 nonsurgical patients did not differ from the 160 operated in clinical, laboratory, or tumor imaging results. The 2 groups did not differ in follow-up time since initial evaluation (range, 11.8-12 years). At surgery, 94% had a tumor removed, 51% were cured immediately, and 41% at last follow-up. Significantly more unoperated patients developed liver metastases (29% vs. 5%, P = 0.0002), died of any cause (54 vs. 21%, P = 0.0002), or died a disease-related death (23 vs. 1%, P < 0.00001). Survival plots showed operated patients had a better disease-related survival (P = 0.0012); however, there was no difference in non-disease-related survival. Fifteen-year disease-related survival was 98% for operated and 74% for unoperated (P = 0.0002).
Conclusions: These results demonstrate that routine surgical exploration increases survival in patients with ZES by increasing disease-related survival and decreasing the development of advanced disease. Routine surgical exploration should be performed in ZES patients.
Figures
References
-
- Fox PS, Hofmann JW, Wilson SD, et al. Surgical management of the Zollinger-Ellison syndrome. Surg Clin North Am. 1974;54:395–407. - PubMed
-
- Oberhelman HA Jr. Excisional therapy for ulcerogenic tumors of the duodenum: long- term results. Arch Surg. 1972;104:447–453. - PubMed
-
- McCarthy DM. The place of surgery in the Zollinger-Ellison syndrome. N Engl J Med. 1980;302:1344–1347. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
