

Leg orientation as a clinical sign for pusher syndrome
- PMID: 16928280
- PMCID: PMC1579228
- DOI: 10.1186/1471-2377-6-30
Leg orientation as a clinical sign for pusher syndrome
Abstract
Background: Effective control of (upright) body posture requires a proper representation of body orientation. Stroke patients with pusher syndrome were shown to suffer from severely disturbed perception of own body orientation. They experience their body as oriented 'upright' when actually tilted by nearly 20 degrees to the ipsilesional side. Thus, it can be expected that postural control mechanisms are impaired accordingly in these patients. Our aim was to investigate pusher patients' spontaneous postural responses of the non-paretic leg and of the head during passive body tilt.
Methods: A sideways tilting motion was applied to the trunk of the subject in the roll plane. Stroke patients with pusher syndrome were compared to stroke patients not showing pushing behaviour, patients with acute unilateral vestibular loss, and non brain damaged subjects.
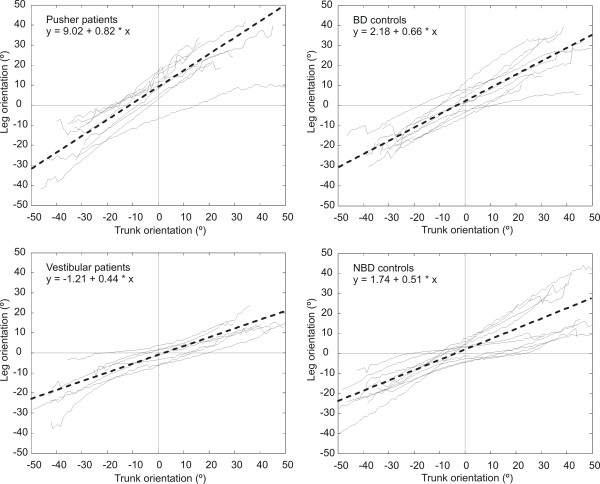
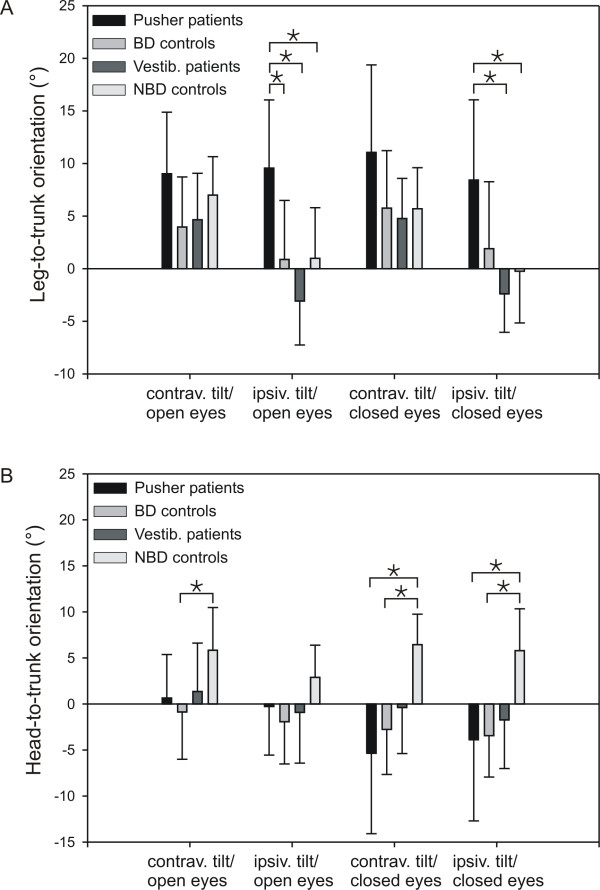
Results: Compared to all groups without pushing behaviour, the non-paretic leg of the pusher patients showed a constant ipsiversive tilt across the whole tilt range for an amount which was observed in the non-pusher subjects when they were tilted for about 15 degrees into the ipsiversive direction.
Conclusion: The observation that patients with acute unilateral vestibular loss showed no alterations of leg posture indicates that disturbed vestibular afferences alone are not responsible for the disordered leg responses seen in pusher patients. Our results may suggest that in pusher patients a representation of body orientation is disturbed that drives both conscious perception of body orientation and spontaneous postural adjustment of the non-paretic leg in the roll plane. The investigation of the pusher patients' leg-to-trunk orientation thus could serve as an additional bedside tool to detect pusher syndrome in acute stroke patients.
Figures

References
-
- Palmer E, Downes L, Ashby P. Associated postural adjustments are impaired by a lesion of the cortex. Neurology. 1996;46:471–475. - PubMed
-
- Wing AM, Goodrich S, Virji-Babul N, Jenner JR, Clapp S. Balance evaluation in hemiparetic stroke patients using lateral forces applied to the hip. Arch Phys Med Rehabil. 1993;74:292–299. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
