

Reducing door-to-antibiotic time in community-acquired pneumonia: Controlled before-and-after evaluation and cost-effectiveness analysis
- PMID: 16928714
- PMCID: PMC2111288
- DOI: 10.1136/thx.2005.056689
Reducing door-to-antibiotic time in community-acquired pneumonia: Controlled before-and-after evaluation and cost-effectiveness analysis
Abstract
Background: Practice guidelines suggest that all patients hospitalised with community-acquired pneumonia (CAP) should receive antibiotics within 4 h of admission. An audit at our hospital during 1999-2000 showed that this target was achieved in less than two thirds of patients with severe CAP.
Methods: An experienced multidisciplinary steering group designed a management pathway to improve the early delivery of appropriate antibiotics to patients with CAP. This was implemented using a multifaceted strategy. The effect of implementation was evaluated using a controlled before-and-after study design over two winter seasons (November-April 2001-2 and 2002-3). Cost-effectiveness analyses were performed from the hospital's perspective.
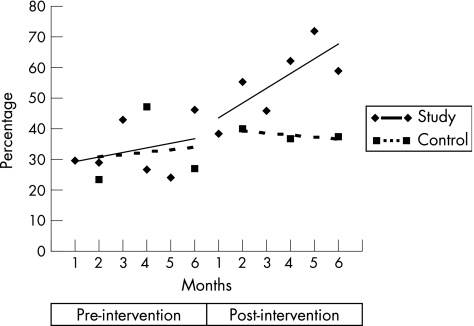
Results: The proportion of patients receiving appropriate antibiotics within 4 h of admission to hospital increased from 33% to 56% at the intervention site, and from 32% to 36% at the control site (absolute change adjusted for differences in severity of illness 17%, p = 0.035). The cost per additional patient receiving appropriate antibiotics within 4 h was 132 pound with no post-implementation evaluation, and 456 pound for a limited post-implementation evaluation. Simple modelling from the results of a large observational study suggests that the cost per death prevented could be 3003 pound with no post-implementation evaluation, or 16,632 pound with a limited post-implementation evaluation.
Conclusions: The intervention markedly improved door-to-antibiotic time, albeit at considerable cost. It might still be a cost-effective strategy, however, to reduce mortality in CAP. Uncertainty about the cost effectiveness of such interventions is likely to be resolved only by a well-designed, cluster randomised trial.
Conflict of interest statement
Competing interests: None.
Comment in
-
Reducing door-to-antibiotic time in community acquired pneumonia.Thorax. 2007 Oct;62(10):925. Thorax. 2007. PMID: 17909196 Free PMC article. No abstract available.
References
-
- Guest J F, Morris A. Community‐acquired pneumonia: the annual cost to the National Health Service in the UK. Eur Resp J 1997101530–1534. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous