

The CURB65 pneumonia severity score outperforms generic sepsis and early warning scores in predicting mortality in community-acquired pneumonia
- PMID: 16928720
- PMCID: PMC2117168
- DOI: 10.1136/thx.2006.067371
The CURB65 pneumonia severity score outperforms generic sepsis and early warning scores in predicting mortality in community-acquired pneumonia
Abstract
Background: The performance of CURB65 in predicting mortality in community-acquired pneumonia (CAP) has been tested in two large observational studies. However, it has not been tested against generic sepsis and early warning scores, which are increasingly being advocated for identification of high-risk patients in acute medical wards.
Method: A retrospective analysis was performed of data prospectively collected for a CAP quality improvement study. The ability to stratify mortality and performance characteristics (sensitivity, specificity, positive predictive value, negative predictive value and area under the receiver operating curve) were calculated for stratifications of CURB65, CRB65, the systemic inflammatory response syndrome (SIRS) criteria and the standardised early warning score (SEWS).
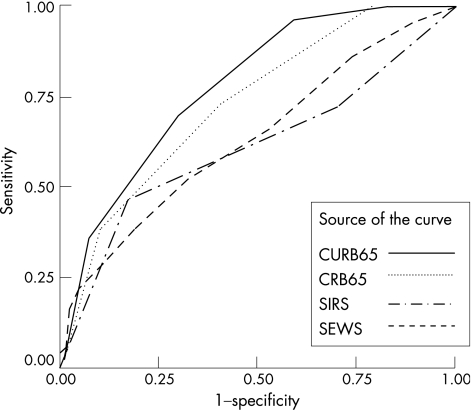
Results: 419 patients were included in the main analysis with a median age of 74 years (men = 47%). CURB65 and CRB65 stratified mortality in a more clinically useful way and had more favourable operating characteristics than SIRS or SEWS; for example, mortality in low-risk patients was 2% when defined by CURB65, but 9% when defined by SEWS and 11-17% when defined by variations of the SIRS criteria. The sensitivity, specificity, positive predictive value and negative predictive value of CURB65 was 71%, 69%, 35% and 91%, respectively, compared with 62%, 73%, 35% and 89% for the best performing version of SIRS and 52%, 67%, 27% and 86% for SEWS. CURB65 had the greatest area under the receiver operating curve (0.78 v 0.73 for CRB65, 0.68 for SIRS and 0.64 for SEWS).
Conclusions: CURB65 should not be supplanted by SIRS or SEWS for initial prognostic assessment in CAP. Further research to identify better generic prognostic tools is required.
Conflict of interest statement
Competing interests: None.
Comment in
-
Simple modification of CURB-65 better identifies patients including the elderly with severe CAP.Thorax. 2007 Nov;62(11):1015-6; author reply 1016. Thorax. 2007. PMID: 17965081 Free PMC article. No abstract available.
-
Mortality predictors are not triage scores.Thorax. 2007 Nov;62(11):1015; author reply 1015. Thorax. 2007. PMID: 17965083 Free PMC article. No abstract available.
References
-
- Jha A K, Li Z, Orav E J.et al Care in US hospitals—the hospital quality alliance program. N Engl J Med 2005353265–274. - PubMed
-
- Mandell L A, Marrie T J, Grossman R F.et al Canadian guidelines for the initial management of community‐acquired pneumonia: an evidence‐based update by the Canadian Infectious Diseases Society and the Canadian Thoracic Society. The Canadian Community‐Acquired Pneumonia Working Group. Clin Infect Dis 200031383–421. - PubMed
-
- American Thoracic Society Guidelines for the management of adults with community‐acquired pneumonia. Am J Respir Crit Care Med 20011631730–1754. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous