

Multiplex ligation-dependent probe amplification: a diagnostic tool for simultaneous identification of different genetic markers in glial tumors
- PMID: 16931583
- PMCID: PMC1867615
- DOI: 10.2353/jmoldx.2006.060012
Multiplex ligation-dependent probe amplification: a diagnostic tool for simultaneous identification of different genetic markers in glial tumors
Abstract
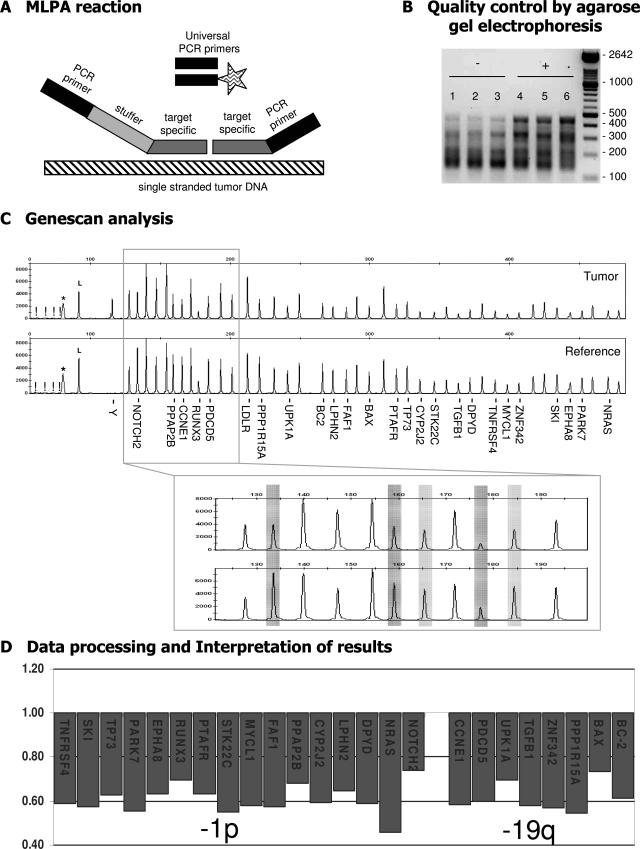
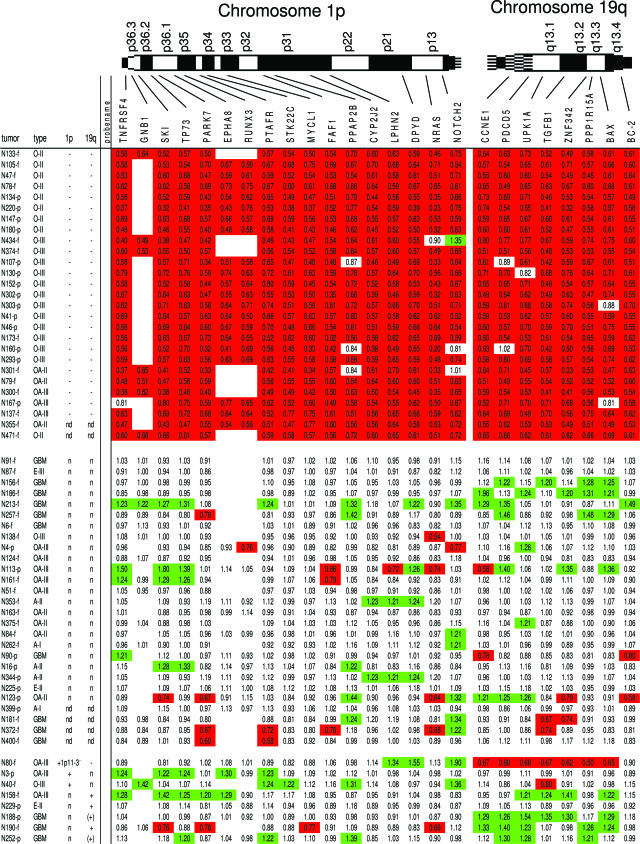
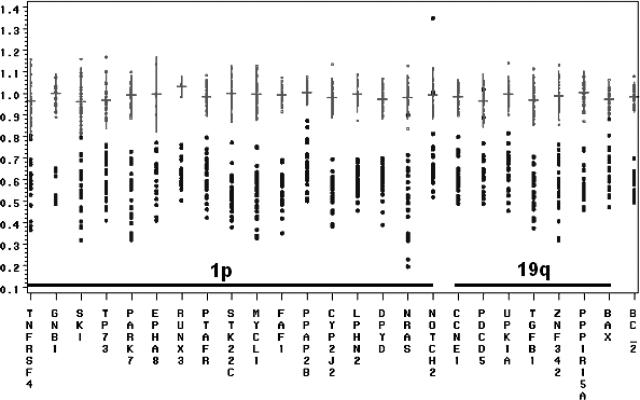
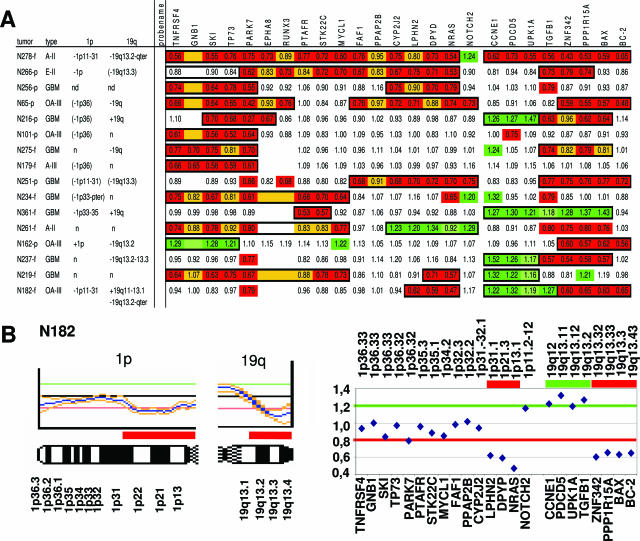
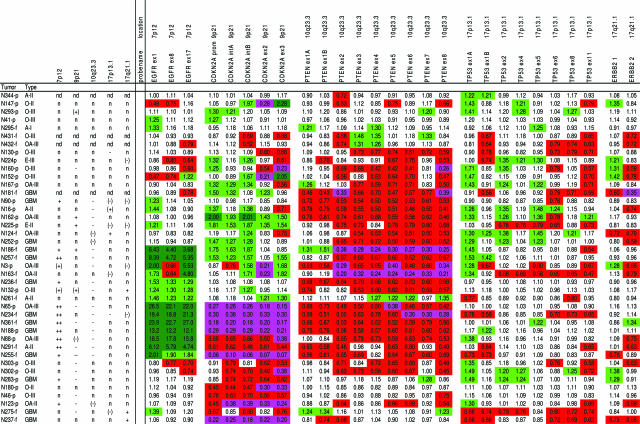
Genetic aberrations in tumors are predictive for chemosensitivity and survival. A test is needed that allows simultaneous detection of multiple changes and that is widely applicable in a routine diagnostic setting. Multiplex ligation-dependent probe amplification (MLPA) allows detection of DNA copy number changes of up to 45 loci in one relatively simple, semiquantitative polymerase chain reaction-based assay. To assess the applicability of MLPA, we performed MLPA analysis to detect relevant genetic markers in a spectrum of 88 gliomas. The vast majority of these tumors (n = 79) were previously characterized by comparative genomic hybridization. With MLPA kit P088 (78 cases), complete and partial loss of 1p and 19q were reliably identified, even in samples containing only 50% tumor DNA. Distinct 1p deletions exist with different clinically prognostic consequences, and in contrast to the commonly used diagnostic strategies (loss of heterozygosity or fluorescent in situ hybridization 1p36), P088 allows detection of such distinct 1p losses. Combining P088 with P105 will further increase the accurate prediction of clinical behavior because this kit identified markers (EGFR, PTEN, and CDKN2A) of high-grade malignancy in 41 cases analyzed. We conclude that MLPA is a reliable diagnostic tool for simultaneous identification of different region-specific genetic aberrations of tumors.
Figures
References
-
- Cairncross JG, Ueki K, Zlatescu MC, Lisle DK, Finkelstein D, Hammond RR, Silver JS, Stark PC, Macdonald DR, Ino Y, Ramsay DA, Louis DN. Specific genetic predictors of chemotherapeutic response and survival in patients with anaplastic oligodendrogliomas. J Natl Cancer Inst. 1998;90:1473–1479. - PubMed
-
- Schmid JS, Perry A, Borell TJ, Lee HK, O’Fallon J, Hosek SM, Kimmel D, Yates A, Burger PC, Scheithauer BW, Jenkins RB. Alterations of chromosome arms 1p and 19q as predictors of survival in oligodendrogliomas, astrocytomas, and mixed oligoastrocytomas. J Clin Oncol. 2000;18:636–645. - PubMed
-
- Cairncross JG. Aggressive oligodendroglioma: a chemosensitive tumor. Recent Results Cancer Res. 1994;135:127–133. - PubMed
-
- Kyritsis AP, Yung WKA, Bruner J, Gealson M, Levin VA. The treatment of anaplastic oligodendrogliomas and mixed gliomas. Neurosurgery. 1993;32:365–371. - PubMed
-
- Nutt CL, Mani DR, Betensky RA, Tamayo P, Cairncross JG, Ladd C, Pohl U, Hartmann C, McLaughlin ME, Batchelor TT, Black PM, von Deimling A, Pomeroy SL, Golub TR, Louis DN. Gene expression-based classification of malignant gliomas correlates better with survival than histological classification. Cancer Res. 2003;63:1602–1607. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
