

Multifocal neoplastic precursor lesions associated with lobular atrophy of the pancreas in patients having a strong family history of pancreatic cancer
- PMID: 16931950
- PMCID: PMC2746409
Multifocal neoplastic precursor lesions associated with lobular atrophy of the pancreas in patients having a strong family history of pancreatic cancer
Abstract
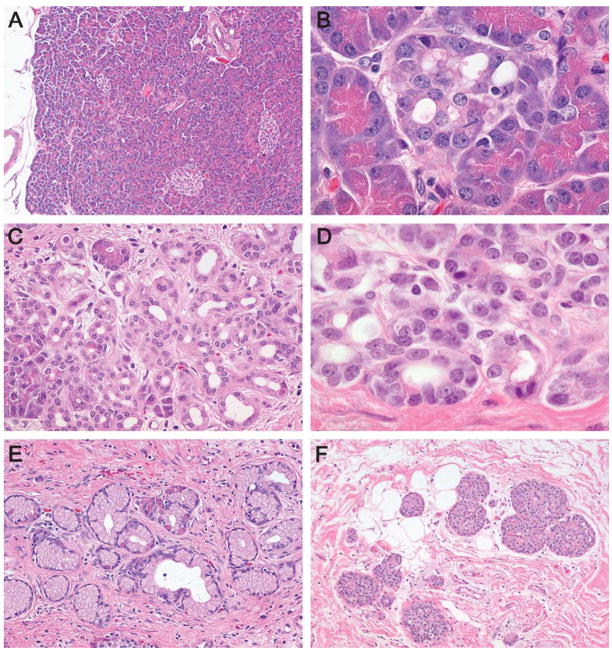
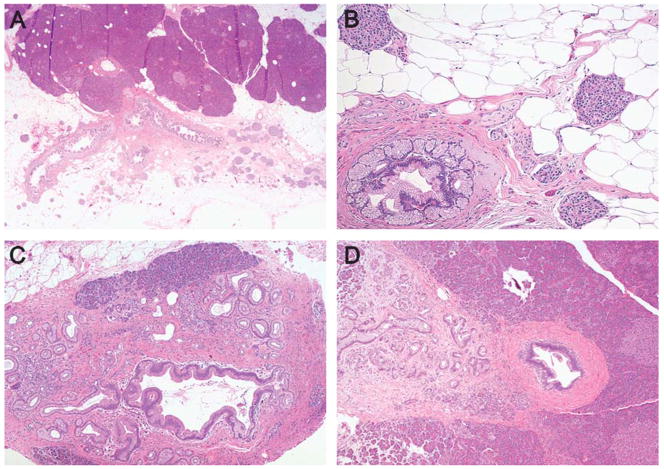
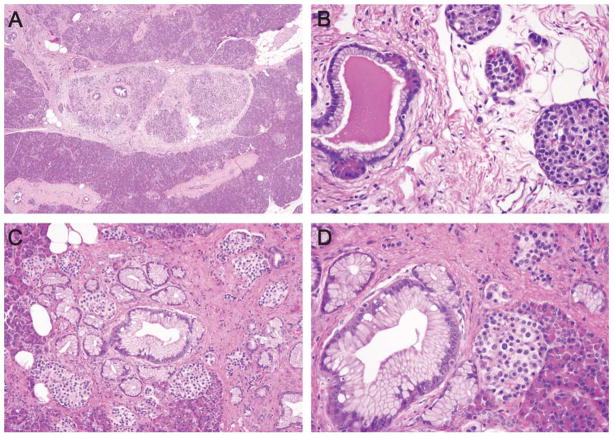
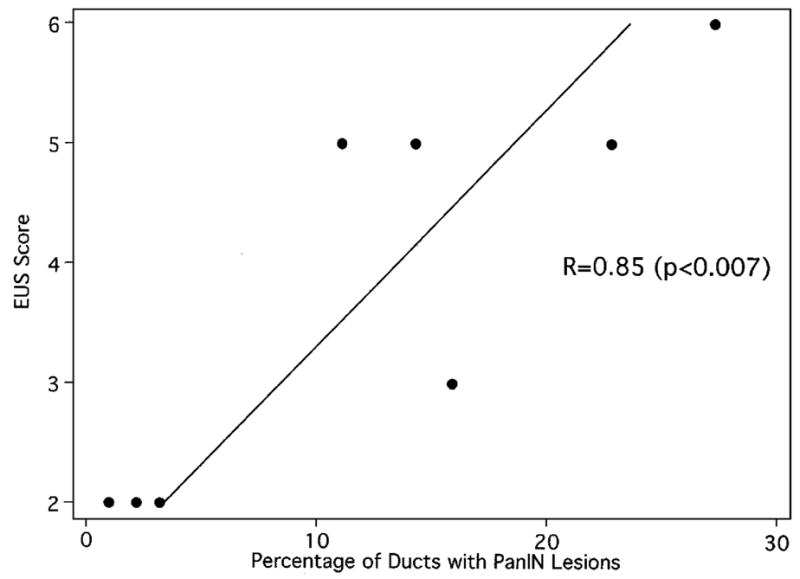
We screened 116 patients with a strong family history of pancreatic cancer using a combination of endoscopic ultrasound and computed tomography. Ten of these patients underwent surgical resection at our institution, providing an opportunity to define the morphology of pancreatic precursor lesions in patients with a strong family history of pancreatic cancer. Eight of the 10 pancreata were available and these were entirely submitted for histologic examination. The number of pancreatic intraepithelial neoplasia (PanIN) lesions and intraductal papillary mucinous neoplasms (IPMNs) were compared with age-matched controls. Parenchymal changes were defined. Selected precursor neoplasms from 6 pancreata were microdissected and analyzed for KRAS gene mutations. PanINs were significantly more common in the 8 cases (mean of 10.7% of the duct profiles, range 1.0% to 27.3%) than in the controls (mean 1.9%, range 0% to 9.2%, P<0.01). Different KRAS gene mutations were identified in separately microdissected precursor lesions in 2 of 6 cases. IPMNs were identified in 4 of the 8 cases, including 2 pancreata each having 2 distinct IPMNs. Both the IPMNs and the PanINs, even the low-grade PanIN-1 lesions, were associated with lobular parenchymal atrophy. Some individuals with a strong family history of pancreatic cancer develop multifocal, noninvasive epithelial precursor lesions of the pancreas. PanINs and IPMNs produce obstructive lobular atrophy, and this atrophy is likely the source of the chronic pancreatitis-like changes seen in these patients. The multifocal nature of familial pancreatic neoplasia suggests that surveillance of these patients is warranted after partial pancreatectomy.
Figures
Comment in
-
Familial and sporadic pancreatic carcinoma, epidemiologic concordance.Am J Surg Pathol. 2007 Apr;31(4):645-6. doi: 10.1097/PAS.0b013e31802d6d42. Am J Surg Pathol. 2007. PMID: 17414117 No abstract available.
References
-
- Arnozan V. Contribution a l’Etude du Pancreas du Lapin. Lesions provoquees par la ligature du canal de Wirsung. Arch Physiol Norm Pathol. 1884;3:287–316.
-
- Beachy PA, Karhadkar SS, Berman DM. Tissue repair and stem cell renewal in carcinogenesis. Nature. 2004;432:324–331. - PubMed
-
- Boerma D, Straatsburg IH, Offerhaus GJ, et al. Experimental model of obstructive, chronic pancreatitis in pigs. Dig Surg. 2003;20:520–526. - PubMed
-
- Boquist L, Edström C. Ultrastructure of pancreatic acinar and islet parenchyma in rats at various intervals after duct ligation. Virchows Arch Abt A Path Anat. 1970;349:69–79. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
