

Administration of antibiotics via the respiratory tract for the prevention of ICU-acquired pneumonia: a meta-analysis of comparative trials
- PMID: 16934148
- PMCID: PMC1750990
- DOI: 10.1186/cc5032
Administration of antibiotics via the respiratory tract for the prevention of ICU-acquired pneumonia: a meta-analysis of comparative trials
Abstract
Introduction: The administration of prophylactic antibiotics via the respiratory tract is one of several strategies for the prevention of ICU-acquired pneumonia. We systematically examined the available evidence regarding the effect of prophylactic antibiotics administered via the respiratory tract on the development of ICU-acquired pneumonia, mortality, colonization of the respiratory tract, emergence of antimicrobial resistance, and toxicity.
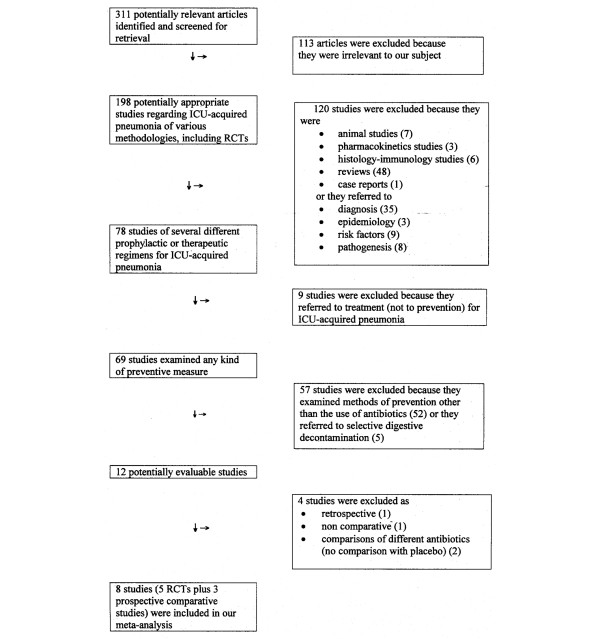
Methods: We searched the PubMed database (1/1950 to 9/2005) and references from relevant articles to identify trials that provided comparative data regarding the above-mentioned outcomes. Two investigators independently performed the data extraction to calculate the effect of the studied intervention on clinically relevant outcomes.
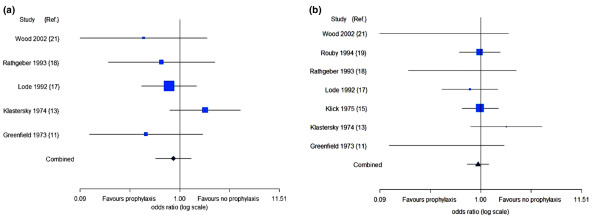
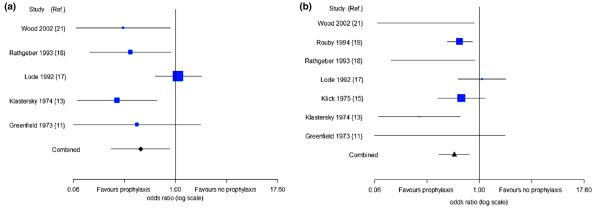
Results: 8 comparative trials (5 randomized controlled trials (RCTs) and 3 non-randomized trials) studying gentamicin (3 trials) polymyxins (3 trials), tobramycin (1 trial), and ceftazidime (1 trial) that studied 1,877 patients were included in our meta-analysis. Our primary analysis that included the 5 RCTs, revealed that ICU-acquired pneumonia was less common in the group of patients that received the antibiotic prophylaxis (OR = 0.49, 95% CI 0.32-0.76). No difference in mortality was found between the compared groups (OR = 0.86, 95% CI 0.55-1.32). There were limited data to permit an analysis of colonization with Pseudomonas aeruginosa. A secondary analysis by adding the 3 non-randomized comparative trials did not reveal substantially different results regarding ICU-acquired pneumonia and mortality, while fewer patients were colonized with Pseudomonas aeruginosa in the group that received prophylaxis, compared to the group of patients that received no prophylaxis (OR = 0.51, 95% CI 0.30-0.86). No serious drug-related toxicity was noted. No meaningful systematic analysis of the evidence regarding the emergence of resistance could be performed in the studies included in our meta-analysis.
Conclusions: The limited available evidence supports that prophylactic administration of antibiotics via the respiratory tract is associated with reduction of occurrence of ICU-acquired pneumonia. However, there is evidence from non-comparative studies that this preventive strategy may lead to an increase in the emergence of resistant bacteria. Thus, further investigation, at least in ICU patients at high risk for development of ICU-acquired pneumonia is warranted, including a more systematic evaluation of issues related to the emergence of resistance.
Figures
Similar articles
-
Effects of prophylactic nebulized antibiotics on the prevention of ICU-acquired pneumonia: a systematic review and meta-analysis.PeerJ. 2024 Dec 13;12:e18686. doi: 10.7717/peerj.18686. eCollection 2024. PeerJ. 2024. PMID: 39686984 Free PMC article.
-
Administration of antimicrobials via the respiratory tract for the treatment of patients with nosocomial pneumonia: a meta-analysis.J Antimicrob Chemother. 2007 Dec;60(6):1216-26. doi: 10.1093/jac/dkm385. Epub 2007 Oct 13. J Antimicrob Chemother. 2007. PMID: 17934205
-
Prevention of ventilator-associated pneumonia, mortality and all intensive care unit acquired infections by topically applied antimicrobial or antiseptic agents: a meta-analysis of randomized controlled trials in intensive care units.Crit Care. 2011 Jun 24;15(3):R155. doi: 10.1186/cc10285. Crit Care. 2011. PMID: 21702946 Free PMC article.
-
Sources of multidrug-resistant Acinetobacter baumannii and its role in respiratory tract colonization and nosocomial pneumonia in intensive care unit patients.Chin Med J (Engl). 2013;126(10):1826-31. Chin Med J (Engl). 2013. PMID: 23673094
-
Antibiotic prophylaxis to prevent nosocomial infections in patients in intensive care units: evidence that struggle to convince practising clinicians.Intern Emerg Med. 2006;1(2):160-2. doi: 10.1007/BF02936546. Intern Emerg Med. 2006. PMID: 17111793 Review.
Cited by
-
Effect of nebulised inhalation of antibiotics on preventing ventilator-associated pneumonia in critically ill patients: a systematic review and meta-analysis.BMJ Open. 2025 May 31;15(5):e093868. doi: 10.1136/bmjopen-2024-093868. BMJ Open. 2025. PMID: 40449947 Free PMC article.
-
Impact of appropriate antimicrobial treatment on transition from ventilator-associated tracheobronchitis to ventilator-associated pneumonia.Crit Care. 2014 Jun 23;18(3):R129. doi: 10.1186/cc13940. Crit Care. 2014. PMID: 24958136 Free PMC article.
-
Effects of prophylactic nebulized antibiotics on the prevention of ICU-acquired pneumonia: a systematic review and meta-analysis.PeerJ. 2024 Dec 13;12:e18686. doi: 10.7717/peerj.18686. eCollection 2024. PeerJ. 2024. PMID: 39686984 Free PMC article.
-
Effect of nebulized eucalyptus on contamination of microbial plaque of endotracheal tube in ventilated patients.Iran J Nurs Midwifery Res. 2016 Mar-Apr;21(2):165-70. doi: 10.4103/1735-9066.178242. Iran J Nurs Midwifery Res. 2016. PMID: 27095990 Free PMC article.
-
Inhaled anti-infective chemotherapy for respiratory tract infections: successes, challenges and the road ahead.Adv Drug Deliv Rev. 2015 May;85:65-82. doi: 10.1016/j.addr.2014.11.004. Epub 2014 Nov 12. Adv Drug Deliv Rev. 2015. PMID: 25446140 Free PMC article. Review.
References
-
- Dodek P, Keenan S, Cook D, Heyland D, Jacka M, Hand L, Muscedere J, Foster D, Mehta N, Hall R, et al. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305–313. - PubMed
-
- Tablan OC, Anderson LJ, Arden NH, Breiman RF, Butler JC, McNeil MM. Guideline for prevention of nosocomial pneumonia. The Hospital Infection Control Practices Advisory Committee, Centers for Disease Control and Prevention. Infect Control Hosp Epidemiol. 1994;15:587–627. - PubMed
-
- Tablan OC, Anderson LJ, Besser R, Bridges C, Hajjeh R. Guidelines for preventing health-care – associated pneumonia, 2003: recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR Recomm Rep. 2004;53:1–36. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
